A 327-person eye-tracking study found that anxiety disorders carried a hyper-scanning and hyper-pursuit signature, separating anxiety patients from healthy controls with AUC 0.82.1 The same eye-movement data separated anxiety from depression poorly, so the result is better read as a behavioral arousal marker than as a ready diagnostic test.
Research Highlights
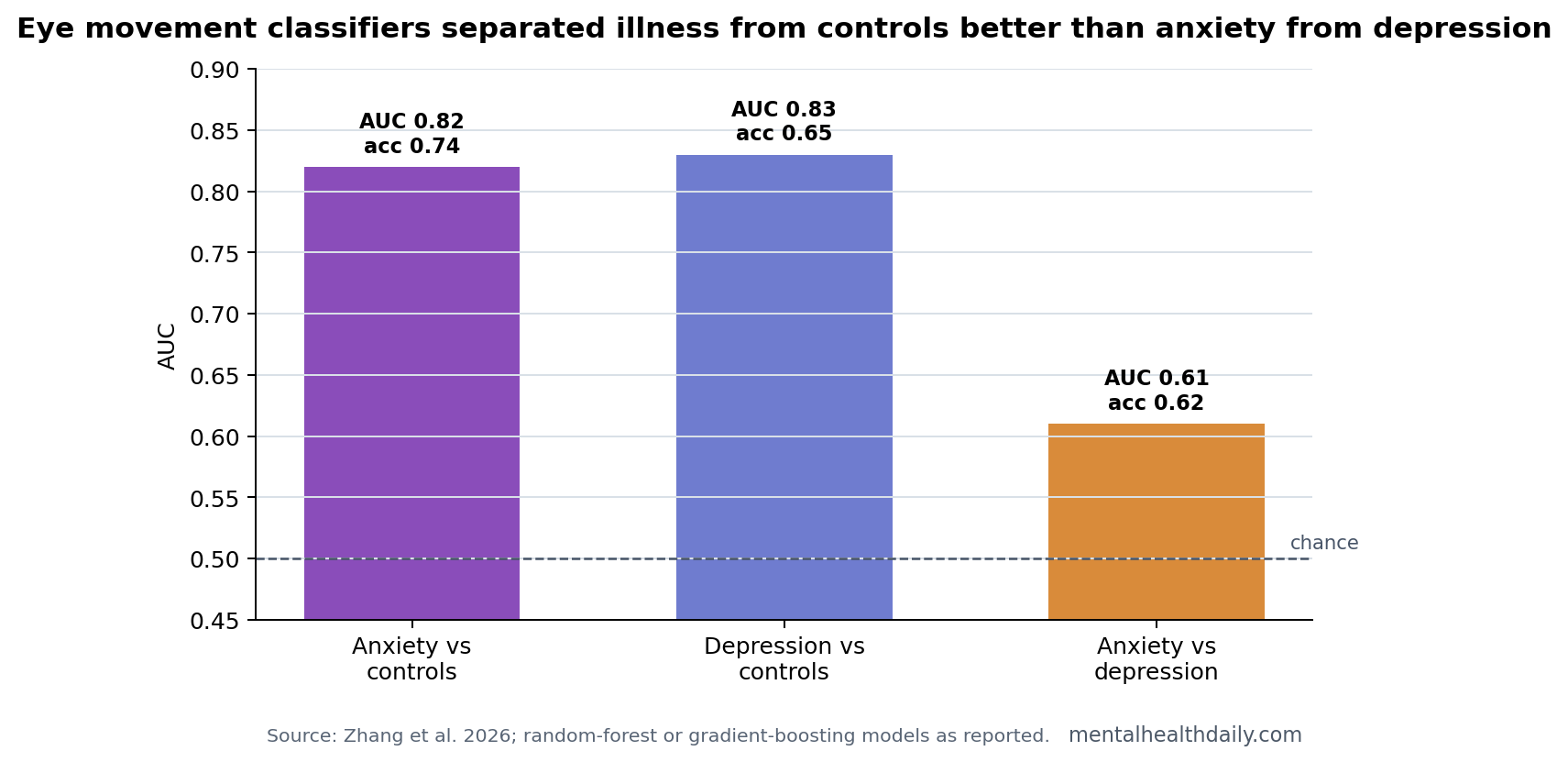
- Anxiety vs controls separated well: Random-forest modeling yielded AUC 0.82, accuracy 0.74, sensitivity 0.77, and specificity 0.71 for anxiety disorders vs healthy controls.1
- Anxiety vs depression barely separated: The best depression-vs-anxiety model reached only AUC 0.61, accuracy 0.62, sensitivity 0.42, and specificity 0.74.1
- Hyper-scanning was visible: Anxiety patients showed more saccades than controls, 18.87 vs. 16.67, and longer scan paths, 108.99 vs. 97.49.1
- Hyper-pursuit also appeared: Anxiety and depression groups showed higher smooth-pursuit velocity gain than controls across multiple pursuit tasks, with vertical gain differing at P < 0.001.1
- Clinical use remains early: A 327-person cross-sectional biomarker study can define a signal; it cannot make eye tracking a stand-alone anxiety diagnosis.
Hyper-scanning means the eyes move more frequently and cover more visual distance during free viewing. In anxiety, that pattern fits hypervigilance: the visual system samples the environment more actively even when the images are neutral rather than threatening.
Hyper-pursuit means stronger-than-usual smooth pursuit gain while tracking a moving target. Smooth pursuit depends on coordinated visual prediction, attention, cerebellar control, and cortical eye-field regulation. It is a behavioral readout of control dynamics, not a symptom rating.
Anxiety Patients Made More Saccades and Longer Scan Paths
Zhang et al. enrolled 91 patients with anxiety disorders, 118 patients with depression, and 118 healthy controls. The anxiety group included generalized anxiety disorder, panic disorder, and social anxiety disorder diagnoses, which makes the result a broad anxiety-disorder signal rather than a single-diagnosis result.1
During free viewing of neutral images, anxiety patients showed more fixations, more saccades, and longer scan paths than both depression patients and healthy controls. Saccade count was 18.87 in the anxiety group vs. 16.67 in controls, P < 0.001. Scan path length was 108.99 vs. 97.49, P = 0.006.1
Interpretation: neutral scenes still produced an over-sampling pattern in anxiety. That supports the idea that anxiety affects baseline attentional style and reactions to obviously threatening images.
Smooth-Pursuit Gain Was Higher in Anxiety and Depression
Smooth pursuit asks the eyes to track a moving target without making jump-like corrections. Higher velocity gain means the eye movement more closely matches or overshoots the moving target’s speed, depending on task context.
Vertical velocity gain differed across groups, F(2,302) = 8.83, P < 0.001. Both anxiety and depression groups showed higher gain than healthy controls. Slow Lissajous horizontal velocity gain showed an even larger group effect, F(2,302) = 18.72, P < 0.001.1
- Anxiety-specific component: free-viewing scan behavior distinguished anxiety from both controls and depression more clearly.
- Shared affective component: pursuit gain rose in anxiety and depression, which weakens diagnostic specificity.
- Mechanistic read: arousal, noradrenergic tone, attentional control, and visual prediction may all contribute.
AUC 0.82 Is Promising; AUC 0.61 Is the Calibration
Area under the receiver operating characteristic curve (AUC) measures how well a model ranks cases above non-cases. AUC 0.50 is chance-level ranking; AUC 1.00 is perfect separation.
The anxiety-vs-control model reached AUC 0.82. That is a meaningful signal for a behavioral marker. The anxiety-vs-depression model reached AUC 0.61, which is only modestly above chance and had low sensitivity at 0.42.1
That pair of results prevents overclaiming. Eye movement signatures appear strong when the comparison is illness vs healthy control. They become much less specific when the comparison is anxiety vs another internalizing disorder.
Eye Tracking Fits Anxiety Biology Better Than Diagnosis Coding
Prior anxiety eye-tracking research often focused on threat bias: faster orientation to threat, difficulty disengaging, or later avoidance.2 The 2026 study tested neutral free viewing and basic pursuit tasks, which means the signal did not require emotional threat cues to appear.
That pattern fits attentional control theory, the idea that anxiety makes attention less efficient by increasing stimulus-driven processing and reducing top-down control.3 Hyper-scanning during neutral viewing is a behavioral version of that theory: the eyes keep sampling, checking, and updating.
The study’s design is useful because neutral viewing removes one easy explanation. If anxiety patients scan more only when they see angry faces, snakes, or threat words, the result could be read mainly as threat bias. More scanning during neutral image viewing suggests a broader attentional-control style that may be present before any obvious threat cue appears.
That broader style also explains why eye tracking could complement symptom scales. A self-report questionnaire asks what the person notices, fears, avoids, or feels. Eye tracking measures where visual attention goes and how the oculomotor system regulates pursuit. Those are related channels, but they are not interchangeable.
Evidence-strength note: this was a cross-sectional biomarker study. It can identify group differences and classifier performance. It cannot show whether eye-movement patterns cause anxiety, result from anxiety, track medication state, or fluctuate with treatment.
Clinical Translation Should Start With Monitoring, Not Diagnosis
The most realistic near-term use is not a clinic telling someone they have anxiety because their saccades are high. A better first use is measurement inside research and treatment trials: eye tracking could test whether attention-control training, exposure therapy, medication, sleep improvement, or neuromodulation changes hyper-scanning and pursuit dynamics.
For diagnosis, specificity is the bottleneck. Anxiety vs depression AUC 0.61 is too weak for stand-alone classification. For mechanism and treatment monitoring, the same signal can still be useful because it captures a quantifiable behavioral channel that symptom scales miss.
Three implementation details decide whether this kind of biomarker becomes useful:
- Task standardization. Free-viewing images, smooth-pursuit targets, fixation calibration, and exclusion rules must be consistent enough that results can be compared across clinics and studies.
- Medication and comorbidity handling. Antidepressants, benzodiazepines, stimulants, sleep loss, depression, and neurological disease can all alter eye movements, so future studies need enough power to separate those effects.
- Longitudinal validation. The marker becomes more clinically useful if saccade count, scan path length, or pursuit gain changes when anxiety improves, relapses, or shifts with treatment.
That is why the 2026 result is best treated as a measurement platform signal. It is stronger than a speculative mechanism claim, but weaker than a diagnostic device claim.
Why Anxiety vs Depression Is the Harder Test
Healthy-control comparisons are useful for discovery, but they are not the clinical problem. In real practice, anxiety commonly overlaps with depression, insomnia, trauma symptoms, substance use, medication effects, and medical illness. A marker that separates patients from healthy controls can still fail when the comparison is another psychiatric group.
The Zhang et al. model showed exactly that calibration problem. Anxiety vs healthy controls reached AUC 0.82, and depression vs healthy controls reached AUC 0.83, but anxiety vs depression reached only AUC 0.61.1 The eye-movement signal is therefore partly a general internalizing-disorder or arousal signal, not a clean anxiety-only signature.
That does not make the result useless. A transdiagnostic marker can still help researchers track arousal, vigilance, attention control, or treatment response across anxiety and depression. It only fails if marketed as a diagnostic shortcut that can replace clinical assessment.
The most honest read is directional: hyper-scanning looks more anxiety-weighted, while altered pursuit gain looks less specific. Future studies should test whether those components split differently across panic disorder, generalized anxiety disorder, social anxiety disorder, major depression, and comorbid presentations.
Replication also needs ordinary clinical controls. Sleep deprivation, caffeine, nicotine, stimulant treatment, benzodiazepines, antidepressant dose, visual acuity, and neurological history can all affect eye movement. A biomarker that survives those checks would be much more convincing than one that works only in a tightly selected laboratory sample.
The field should therefore treat AUC 0.82 as a discovery signal and AUC 0.61 as the guardrail. The first number says the oculomotor system carries anxiety-relevant information. The second number says that psychiatric specificity is still the unsolved problem.
For a patient-facing technology, that distinction is crucial. A clinic could eventually use eye tracking as one objective measurement among many, especially for treatment monitoring or research stratification. It would be much riskier to present a brief eye-tracking task as a binary anxiety test when depression and anxiety share so much oculomotor signal.
Questions About Eye Movement Biomarkers for Anxiety
Can eye tracking diagnose anxiety disorders?
No. In this study, anxiety vs healthy-control separation was strong, but anxiety vs depression separation was weak. Clinical diagnosis still requires history, symptoms, impairment, differential diagnosis, and context.
What does hyper-scanning mean in plain English?
It means the eyes jump and scan more. In anxiety, that can reflect an overactive checking style even when the scene does not contain an obvious threat.
Could this be useful in treatment studies?
Yes. If a treatment reduces symptoms and normalizes scan path length, saccade count, or pursuit gain, that could give researchers an objective behavioral marker alongside self-report scales.
References
- Zhang Y, et al. Hyper-scanning and hyper-pursuit define eye movement biomarkers of anxiety disorders. British Journal of Psychiatry. 2026. doi:10.1192/bjp.2026.10626
- Armstrong T, Olatunji BO. Eye tracking of attention in the affective disorders: a meta-analytic review and synthesis. Clinical Psychology Review. 2012. PubMed
- Eysenck MW, Derakshan N, Santos R, Calvo MG. Anxiety and cognitive performance: attentional control theory. Emotion. 2007. PubMed
- Levy DL, et al. Eye tracking dysfunction and schizophrenia: clinical and neurobiological implications. Schizophrenia Bulletin. PubMed