A 2026 case series of 5 adults with bodily distress disorder found mean pain scores decreased from 9.0 to 3.8 after accelerated transcranial direct current stimulation, with 4 of 5 patients achieving at least 50% pain reduction.1 The result is a feasibility signal, not proof of efficacy, because every patient knew they were receiving stimulation and medications continued during treatment.
Research Highlights
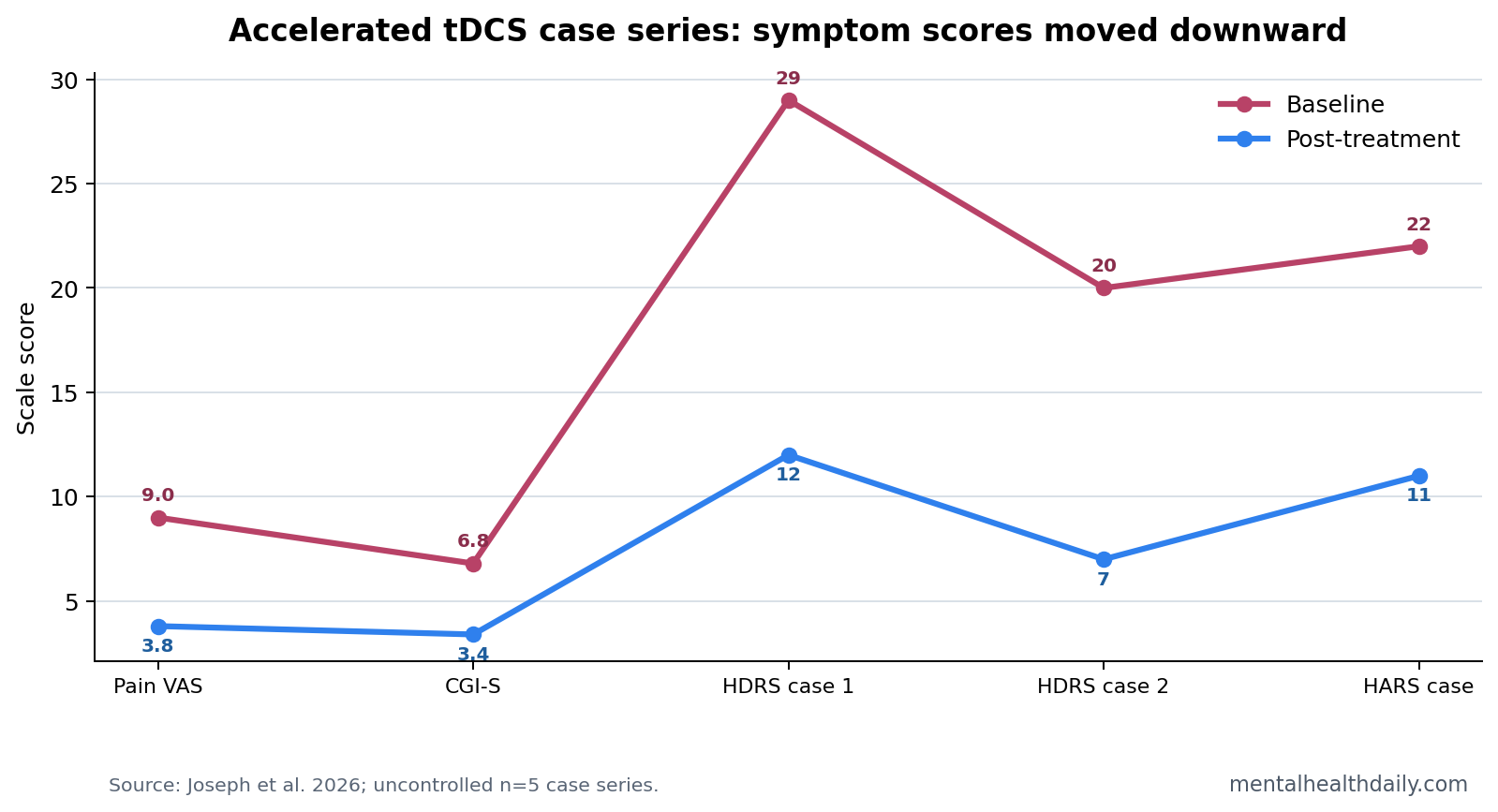
- Pain scores fell quickly: Mean visual analogue scale pain decreased from 9.0 to 3.8 after accelerated tDCS in 5 cases.1
- Most cases met response criteria: 4 of 5 patients had at least 50% pain reduction, and the same 4 met Clinical Global Impression response criteria.1
- Severity improved: Mean CGI-S scores decreased from 6.8 to 3.4, shifting the group from severe illness toward moderate symptoms.1
- The schedule was intensive: Patients received a mean of 22 sessions over 7 to 12 days, usually at 2 mA for 20 minutes.1
- Evidence remains weak: The report included 5 uncontrolled cases, so placebo response, regression to the mean, attention, and medication effects remain live explanations.1
Bodily distress disorder describes persistent physical symptoms that cause disability and distress even when routine medical testing does not fully explain the symptom burden. The diagnosis is clinically difficult because pain, fatigue, gastrointestinal symptoms, anxiety, depression, substance use, sleep disturbance, and prior medical workups often sit in the same patient.
Transcranial direct current stimulation (tDCS) delivers weak electrical current through scalp electrodes to shift cortical excitability. In this case series, the researchers mostly placed the anode over the left motor cortex, a common pain-modulation target, and clustered multiple sessions per day into an accelerated schedule.
4 of 5 Patients Had at Least 50% Pain Reduction
Joseph et al. treated 5 adults aged 43 to 50 years with moderate to severe bodily distress disorder. Illness duration ranged from 1 to 15 years, and 3 patients had already failed at least 2 pharmacological treatments. Four patients received left motor cortex stimulation, while 1 patient with prominent anxiety received bilateral dorsolateral prefrontal cortex stimulation.1
The primary symptom signal was pain. Mean visual analogue scale scores decreased from 9.0 to 3.8, and 4 patients crossed the predefined response threshold of at least 50% pain reduction. CGI-S scores improved from 6.8 to 3.4.
The tDCS Schedule Was More Like a Burst Than Standard Weekly Treatment
The intervention was not a typical slow outpatient neuromodulation course. Patients received 2 to 5 sessions per day, spaced 1 to 2 hours apart, with 20 to 25 total sessions over 7 to 12 days. Stimulation used 2 mA for 20 minutes per session, with 30 seconds of ramp-up and ramp-down.
- Motor-cortex target: 4 patients received anodal stimulation over C3, corresponding to left primary motor cortex, with the cathode over FP2.
- Prefrontal target: 1 patient received left-anodal and right-cathodal dorsolateral prefrontal stimulation because anxiety and nonspecific pain dominated the presentation.
- Adjunctive design: medications continued during the stimulation course, so the case series tested add-on feasibility rather than tDCS alone.
Depression and Anxiety Scores Also Moved in the Responders
Comorbid symptoms improved in the small subset where rating scales were used. Among patients with depression ratings, Hamilton Depression Rating Scale scores dropped by 58.6% and 65%. The patient with anxiety ratings had a 50% reduction on the Hamilton Anxiety Rating Scale.1
Those changes fit the clinical overlap in bodily distress disorder: pain reduction, mood improvement, sleep improvement, and lower threat monitoring can reinforce each other. They do not prove the stimulation directly treated depression or anxiety. The study was too small and uncontrolled for that.
Case-Series Evidence Cannot Estimate the True tDCS Effect
Evidence-strength note: a 5-patient case series can show feasibility, tolerability, and a signal worth testing. It cannot separate active stimulation from nonspecific care, expectancy, medication effects, spontaneous symptom fluctuation, or regression to the mean.
Mechanistic context: prior tDCS studies in chronic pain and fibromyalgia provide a plausible mechanism for motor-cortex stimulation in pain modulation.2 Accelerated psychiatric tDCS reports also make the clustered schedule plausible.4
The next useful test is a sham-controlled trial in bodily distress disorder with stable medication rules, daily pain measures, follow-up after the treatment week, and adverse-event monitoring.
Baseline stability also matters: several pre-treatment daily scores would show whether pain was already drifting before stimulation started.
Which Patients Looked Most Compatible With the Signal?
The responder pattern was not random enough to ignore, but the case series is too small for subgroup claims. The 4 responders had prominent pain or somatic distress and did not have the same degree of complicating substance-use comorbidity as the nonresponder. The single nonresponder had opioid dependence, sedative-hypnotic-anxiolytic dependence, harmful use of non-psychoactive substances, and poor duloxetine compliance.
Clinical interpretation: accelerated tDCS may be easier to test in bodily distress disorder when symptoms are stable enough to measure, medication exposure is documented, substance-use confounding is limited, and daily pain ratings can track change across the stimulation week.
That does not exclude complex patients. It means future trials need stratification. A trial that mixes opioid dependence, sedative use, treatment-resistant depression, anxiety, fibromyalgia-like pain, abdominal pain, headache, and nonspecific burning sensations without prespecified subgroups will be hard to interpret even if the average score improves.
Why Motor-Cortex Stimulation Is Plausible for Somatic Symptoms
The motor cortex is also a pain-modulation node. It connects with thalamic, sensory, affective, and descending pain-control systems. Noninvasive stimulation over motor cortex has been studied for neuropathic pain, fibromyalgia, and other chronic pain states because changing cortical excitability may shift pain amplification and inhibitory control.
Descending pain modulation refers to brainstem and spinal pathways that can turn pain signaling up or down. In chronic pain and bodily distress presentations, the problem is often not a single damaged tissue source. It is an overactive threat-and-pain system that keeps generating distress from bodily signals.
The prefrontal target used in 1 patient reflects a different logic. The dorsolateral prefrontal cortex is involved in cognitive control, threat appraisal, and emotion regulation. For a patient whose bodily distress is dominated by anxiety and diffuse pain, prefrontal stimulation may be a reasonable target, but that single case cannot compare motor cortex vs. prefrontal cortex.
A Good Trial Would Need More Than Pain Scores
Pain VAS is a useful daily outcome because it is simple and sensitive to short-term change. Bodily distress disorder needs a wider endpoint set. Future trials should track somatic symptom burden, disability, sleep, medication changes, health-care use, adverse events, and follow-up durability after the accelerated week ends.
- Primary endpoint: daily pain or somatic symptom severity with a prespecified responder definition.
- Functional endpoint: activity level, work/school functioning, or days spent seeking urgent reassurance or medical care.
- Durability endpoint: symptom scores at 2 weeks, 1 month, and 3 months after stimulation.
- Safety endpoint: skin irritation, headache, dizziness, mood activation, sleep disruption, and discontinuation.
Sham stimulation is especially important in accelerated protocols because the treatment is intense, novel, and delivered with repeated clinical contact. Those features can produce real symptom improvement even when the stimulation itself adds little.
Medication Continuation Makes the Result More Realistic and Less Clean
The case series kept patients on current medications. That choice makes the report clinically realistic because many people with bodily distress disorder are already taking antidepressants, anxiolytics, analgesics, or sleep medications. It also makes the active ingredient harder to isolate.
Interpretation problem: if duloxetine, paroxetine, desvenlafaxine, clinical attention, daily monitoring, and accelerated tDCS all move during the same treatment window, a short-term score drop cannot be assigned to stimulation alone. A controlled trial would need stable medication periods before stimulation starts, or a design that explicitly tests tDCS as add-on therapy.
The accelerated schedule also changes adherence math. Conventional neuromodulation can fail because patients cannot attend weeks of sessions. A 7- to 12-day burst is easier for some patients and harder for others. Feasibility should include tolerability, travel burden, cost, missed work, and whether symptom gains persist after the concentrated clinical contact ends.
Durability is the missing practical variable. A rapid 1-week improvement is meaningful for patients in severe distress, but bodily distress disorder is usually chronic. If pain returns quickly, accelerated tDCS may function as a short rescue intervention. If gains persist, it becomes a more serious candidate for stepped-care trials.
Follow-up target: trials should test whether pain reduction persists after clinical contact drops back to ordinary care.
Questions About Accelerated tDCS for Bodily Distress Disorder
Was the treatment safe in these 5 cases?
No serious adverse events or discontinuations were reported. Mild tingling, itching, burning, and skin redness occurred.
Does this prove tDCS treats bodily distress disorder?
No. The case series supports feasibility and short-term symptom improvement. It does not prove efficacy without a sham comparison.
Why target the motor cortex for bodily distress disorder?
Motor-cortex stimulation is used in pain neuromodulation because the motor cortex connects with thalamic, sensory, and descending pain-control pathways. In this case series, the target was a pain-modulation strategy rather than a claim that bodily distress disorder is a motor-cortex disease.
References
- Joseph J, et al. Accelerated Transcranial Direct Current Stimulation as Adjunctive Treatment for Bodily Distress Disorder: A Case Series. Indian Journal of Psychological Medicine. 2026. doi:10.1177/02537176261442676
- Motor-cortex tDCS for chronic pain systematic reviews. PubMed
- tDCS for fibromyalgia randomized trials and reviews. PubMed
- Accelerated tDCS psychiatric case reports. PubMed