A 2026 Egyptian study of 76 children found a sharp mental-health gradient in phenylketonuria (PKU): late-diagnosed children had higher depression scores, lower quality of life, lower IQ, and a 21.4% rate of reported suicidal thoughts. Early-diagnosed children still differed from controls on some functioning measures, but the late-diagnosed group carried the heaviest psychiatric and cognitive burden.1
Research Highlights
- 76 children were studied: Abuelela et al. compared 22 early-diagnosed PKU children, 28 late-diagnosed PKU children, and 26 healthy controls aged 8-15 years.1
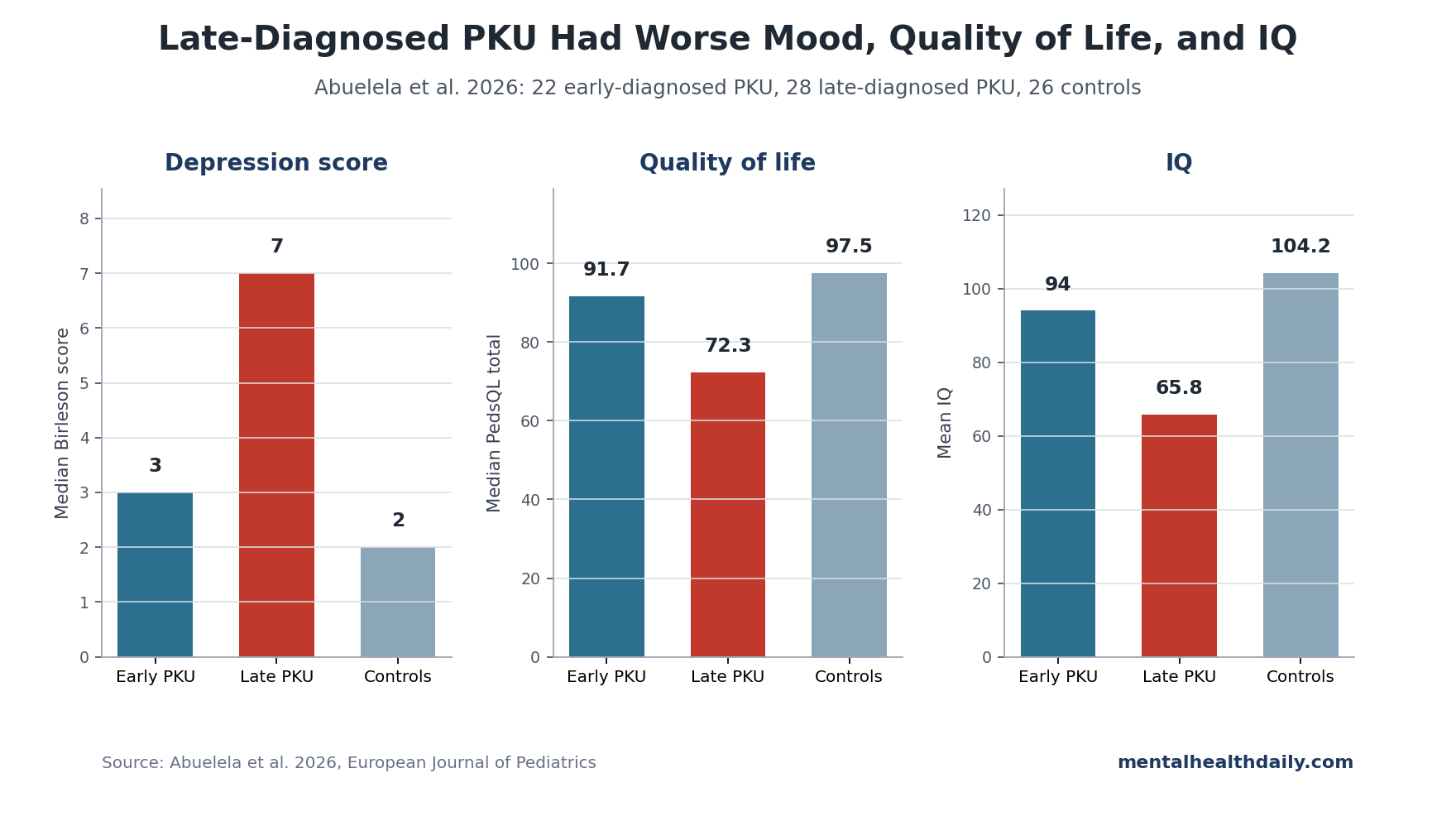
- Late diagnosis tracked higher depression: median Birleson depression score was 7 in late-diagnosed PKU, 3 in early-diagnosed PKU, and 2 in controls, p = 0.001.1
- Suicidal thoughts appeared only in late-diagnosed PKU: 21.4% of late-diagnosed children endorsed suicidal thoughts, compared with 0% in early-diagnosed children and controls.1
- Quality of life was lowest in late-diagnosed children: median total PedsQL score was 72.3 in late-diagnosed PKU, 91.7 in early-diagnosed PKU, and 97.5 in controls.1
- IQ strongly tracked quality of life: total quality of life correlated positively with IQ (r = 0.74) and negatively with depression score (r = −0.51).1
Phenylketonuria is a genetic disorder of phenylalanine hydroxylase (PAH), the enzyme needed to convert phenylalanine into tyrosine. Without early dietary control, phenylalanine can accumulate and disrupt brain development, cognition, mood, and daily functioning.2,3
Abuelela et al. Compared Early-Diagnosed and Late-Diagnosed PKU
The study enrolled 50 children with classical PKU and 26 age- and sex-matched controls. The PKU group was split by diagnosis timing: 22 children were early-diagnosed, and 28 were late-diagnosed. All participants were 8-15 years old.1
Children completed the Birleson Depression Self-Rating Scale for Children (DSRS-C), a self-report depression scale, and the Pediatric Quality of Life Inventory (PedsQL 4.0), which measures physical, emotional, social, and school functioning. IQ was measured with the Stanford-Binet Intelligence Scale.
- PKU cases: 50 children with classical PKU on a phenylalanine-restricted diet.
- Early-diagnosed group: 22 children.
- Late-diagnosed group: 28 children.
- Controls: 26 healthy children.
- Phenylalanine tracking: the researchers used the test-day phenylalanine level and the median level from the prior year.
The design was cross-sectional, so it measured associations at one time point. It cannot prove that late diagnosis alone caused every mood or quality-of-life difference. The group gradient is still clinically meaningful because PKU biology, diagnosis timing, metabolic control, IQ, and depression all pointed in the same direction.
Depression Scores Were Highest in Late-Diagnosed PKU
Median depression score was lowest in controls, intermediate in early-diagnosed PKU, and highest in late-diagnosed PKU:
- Controls: 2 (IQR 0-5).
- Early-diagnosed PKU: 3 (IQR 1-7).
- Late-diagnosed PKU: 7 (IQR 5-9).
- Overall group difference: p = 0.001.
Four late-diagnosed children, or 14.3%, scored in the 11-17 range on the depression scale. No early-diagnosed children or controls fell into that range.1
The symptom pattern extended beyond a small shift in total score. Late-diagnosed children showed high rates of specific depressive symptoms:
- Loss of energy: 85.7%.
- Irritability: 78.6%.
- New somatic complaints: 64.3%.
- Suicidal thoughts: 21.4%.
- Depression delusion: 71.4%.
Those symptom frequencies should be interpreted cautiously because the late-diagnosed group had only 28 children. Even with that caution, the pattern is not subtle. Loss of energy, irritability, new somatic complaints, and suicidal thoughts all clustered in the group with later diagnosis and lower IQ.
The early-diagnosed group did not look identical to controls. Early-diagnosed children differed from controls on reduced activity, p = 0.004, and had lower mean IQ than controls. Early treatment appears protective, but it does not erase the need for developmental and mental-health follow-up.
Quality of Life and IQ Fell With Late Diagnosis
The quality-of-life gap was large. Median total PedsQL score was 97.5 in controls, 91.7 in early-diagnosed PKU, and 72.3 in late-diagnosed PKU. School functioning was especially low in late-diagnosed children: median 50, compared with 90 in early-diagnosed PKU and 100 in controls.1
IQ showed the same timing gradient:
- Controls: mean IQ 104.2.
- Early-diagnosed PKU: mean IQ 94.0.
- Late-diagnosed PKU: mean IQ 65.8.
- Overall group difference: p < 0.001.
This does not make depression a simple IQ proxy. Depression score and IQ were both related to quality of life, and the regression model suggested they added explanatory power beyond diagnosis timing and phenylalanine level.
School functioning may be the clearest everyday signal. Median school score was 50 in late-diagnosed PKU, far below the early-diagnosed group and controls. For a child, that number represents more than test performance. It can reflect attention, fatigue, diet burden, social participation, self-confidence, and the ability to keep up with classroom demands.
Phenylalanine, Depression, and IQ Predicted Quality of Life
The correlation table gives the more technical view. Total quality of life correlated negatively with median phenylalanine level (r = −0.32) and depression score (r = −0.51), and positively with IQ (r = 0.74). In plain terms: higher phenylalanine and higher depression tracked worse quality of life, but higher IQ tracked better quality of life.1
The hierarchical regression model strengthened that pattern:
- Diagnosis timing and phenylalanine: the first model explained 35.0% of quality-of-life variance.
- Depression added information: adding depression increased explained variance to 44.2%.
- IQ added more: adding IQ increased explained variance to 61.3%.
This is the most useful interpretation for care. PKU mental-health burden was tied to metabolic disease rather than floating separately as “poor mood.” In this sample, mood, cognition, metabolic control, and daily functioning were connected.
The phenylalanine correlations were moderate rather than overwhelming. Median phenylalanine correlated with total quality of life at r = −0.32 and with depression at r = 0.40. Those are meaningful associations, but they leave room for family support, diet access, school accommodations, stigma, socioeconomic factors, and psychiatric vulnerability.
That is why a narrow “lower phenylalanine and everything else follows” approach is incomplete. Phenylalanine control is foundational, but it should be paired with mental-health screening, cognitive assessment, and practical support for diet adherence.
Newborn Screening Remains the Main Prevention Lever
PKU is one of the clearest examples where early detection can prevent severe neurological harm. European guidelines emphasize early diagnosis, lifelong treatment, and phenylalanine control, but the psychiatric and quality-of-life outcomes remain uneven even among treated patients.3,6
The Egyptian context is relevant because national newborn screening for PKU began in November 2015. Late-diagnosed children in this study were older and more likely to have rural residence and lower maternal education, which may reflect access and timing barriers rather than biology alone.1
Diagnosis timing also changes what treatment has to accomplish. Early-diagnosed children need prevention of long-term neuropsychiatric burden. Late-diagnosed children may need rehabilitation, school support, depression assessment, family education, and monitoring for suicidal ideation in addition to metabolic care.
Care planning should therefore include 4 parallel targets:
- Earlier diagnosis: newborn screening and fast diet initiation reduce prolonged high phenylalanine exposure.
- Metabolic follow-up: repeated phenylalanine monitoring remains central, not optional.
- Cognitive support: school planning and neuropsychological assessment are part of PKU care.
- Mental-health screening: depression and suicidal thoughts need direct assessment, especially in late-diagnosed children.
PKU Depression Screening Should Be Routine, Not Exceptional
The study used a depression self-report scale rather than a structured psychiatric interview, but the suicidal-thought signal makes screening difficult to ignore. Pediatric PKU follow-up often focuses on phenylalanine levels, diet formulas, growth, and cognition. Mood can get treated as secondary unless it is assessed directly.
A practical screening workflow would include:
- Depressive symptoms: low mood, irritability, sleep change, energy loss, self-deprecating ideas, and somatic complaints.
- Suicide risk: direct questions about suicidal thoughts, especially in late-diagnosed children or children with high depression scores.
- School functioning: attendance, learning support, peer problems, and fatigue during class.
- Diet burden: adherence barriers, food access, family strain, and stigma around special dietary needs.
This does not require turning every metabolic clinic into a psychiatry clinic. It does require a pathway: screen, identify risk, refer, and coordinate with school and family supports.
That pathway is especially important when families are already managing diet restrictions, follow-up blood tests, and school concerns at the same time.
Limitations of the PKU Depression Study
- Small single-center sample. The study included 50 PKU children from one clinic and 26 controls, so estimates need replication in larger cohorts.
- Cross-sectional design. Associations cannot prove the time sequence among phenylalanine, IQ, depression, and quality of life.
- Self-reported depression scale. The Birleson scale can screen depressive symptoms, but it is not the same as a structured psychiatric diagnosis.
- Socioeconomic confounding. Rural residence and maternal education differed across groups, and those factors can affect diagnosis timing, diet adherence, schooling, and mental-health support.
Questions About Depression in Children With PKU
Why did late diagnosis change the mental-health concern?
Late diagnosis meant longer exposure to high phenylalanine during brain development. In this 76-child study, that group had lower IQ, lower quality of life, higher depression scores, and the only reported suicidal thoughts.
Which children had the highest depression scores?
Late-diagnosed children had the highest median depression score: 7, compared with 3 in early-diagnosed PKU and 2 in controls.
Were suicidal thoughts reported?
Yes. Suicidal thoughts were reported in 21.4% of late-diagnosed children and 0% of early-diagnosed children and controls in this sample.
Does early diagnosis remove all risk?
No. Early-diagnosed children looked better than late-diagnosed children, but some differences from controls remained. Early diagnosis reduces risk while long-term metabolic, cognitive, and mental-health follow-up remains necessary.
References
- Abuelela IS, Bebars GM, Kamal AM, Sayed SI, Refaat RS. Impact of depression on quality of life in PKU children. European Journal of Pediatrics. 2026;185:293. doi:10.1007/s00431-026-06933-3
- Blau N, van Spronsen FJ, Levy HL. Phenylketonuria. Lancet. 2010;376:1417-1427. doi:10.1016/s0140-6736(10)60961-0
- van Wegberg AMJ, MacDonald A, Ahring K, et al. The complete European guidelines on phenylketonuria: diagnosis and treatment. Lancet Diabetes & Endocrinology. 2017;5:743-756. doi:10.1016/s2213-8587(16)30320-5
- Vockley J, Andersson HC, Antshel KM, et al. Phenylalanine hydroxylase deficiency: diagnosis and management guideline. Genetics in Medicine. 2014;16:188-200. doi:10.1038/gim.2013.157
- Sharman R, Sullivan K, Young RM, McGill J. Depressive symptoms in adolescents with early and continuously treated phenylketonuria. Gene. 2012;504:288-291. doi:10.1016/j.gene.2012.05.007
- Bilder DA, Noel JK, Baker ER, et al. Systematic review and meta-analysis of neuropsychiatric symptoms in PKU. Developmental Neuropsychology. 2016;41:245-260. doi:10.1080/87565641.2016.1243109
- Becsei D, Hiripi R, Kiss E, et al. Quality of life in children living with PKU: a single-center cross-sectional observational study from Hungary. Molecular Genetics and Metabolism Reports. 2021;29:100823. doi:10.1016/j.ymgmr.2021.100823
- Brumm VL, Bilder D, Waisbren SE. Psychiatric symptoms in phenylketonuria. Molecular Genetics and Metabolism. 2010;99:S59-S63. doi:10.1016/j.ymgme.2009.10.182