
A 2026 machine-learning analysis of 110 adults with generalized anxiety disorder predicted 2-week digital mindfulness engagement with R2 = 82.1% in a top-10 predictor model, and the model favored mindfulness prompts over self-monitoring prompts for engagement (d = 1.447, p < .001).1 The calibrated read is that engagement with brief app-based mindfulness may be matchable, but the matching rule is not ready for clinical assignment without external validation.
Research Highlights
- Prediction was strong internally: A top-10 random-forest model predicted log-transformed prompt completion with R2 = 82.1%, RMSE = 0.547, and MAE = 0.307 in 5-fold nested cross-validation.1
- Mindfulness beat monitoring for engagement: Conditional average treatment engagement favored the mindfulness ecological momentary intervention over self-monitoring by d = 1.447, p < .001.1
- Strengths and deficits both mattered: Higher attentional control, verbal fluency, and empathy predicted more mindfulness engagement, but lower working memory, lower trait mindfulness, and lower expectancy also predicted more engagement.1
- Engagement was narrow: The outcome was completed prompts across 14 days, with 5 prompts per day and 70 possible raw completions, not long-term adherence or symptom remission.1
- Clinical use remains provisional: The model was built in 110 mostly young, predominantly female and White participants, so it needs independent replication before it can guide treatment matching.1
Generalized anxiety disorder is defined by excessive, hard-to-control worry plus symptoms such as restlessness, fatigue, concentration difficulty, irritability, muscle tension, and sleep disturbance. Digital mindfulness tools try to interrupt that loop by prompting attention to present experience, slower breathing, and nonjudgmental observation in daily life rather than only during weekly therapy visits.
Mindfulness ecological momentary intervention (MEMI) means a brief mobile-phone intervention delivered inside ordinary routines. In this trial, the mindfulness arm received 5 daily prompts for 14 days, including brief exercises built around diaphragmatic breathing, present-mindedness, and nonjudgmental acceptance. The comparison arm used self-monitoring: participants rated distress and thoughts on the same schedule, but the app did not teach mindfulness skills or breathing practice.1
110 Adults With GAD Received Mindfulness or Self-Monitoring Prompts
Zainal and Newman analyzed data from a randomized trial involving 110 adults diagnosed with generalized anxiety disorder by structured interview. The mindfulness arm included 68 participants, and the self-monitoring arm included 42. Participants averaged 20.80 years old, and the sample was 88.67% women, 64.55% White, 13.63% Asian, 7.27% Hispanic, and 5.45% African American.1
The engagement outcome was simple: how many prompts each participant completed during the 2-week protocol. With 5 prompts per day over 14 days, the raw count could range from 0 to 70. Researchers log-transformed that count because completion was left-skewed; the mean log-transformed engagement score was 4.30, with SD = 1.03 and a 0 to 4.62 range.1
Random forest is a machine-learning method that builds many decision trees and averages their predictions. The study used 5-fold nested cross-validation, meaning model tuning and model testing were separated so the algorithm could not learn from the same data used to evaluate it. That safeguard matters in a small trial because flexible models can otherwise memorize noise and look better than they are.
The Top-10 Model Explained 82.1% of Prompt Completion Variance
The initial 16-predictor model included age, sex, race, attentional control, inhibition, set-shifting, verbal fluency, working memory, executive dysfunction, trait mindfulness, empathy, treatment credibility or expectancy, depression symptoms, GAD severity, and repetitive negative thinking. It predicted engagement with R2 = 82.7%, but the 95% confidence interval was wide: 15.9% to 97.5%.1
The pared-down top-10 model kept almost the same R2, at 82.1%, while narrowing uncertainty to 75.0% to 87.4%. Error also improved: RMSE fell from 0.780 to 0.547, and MAE fell from 0.512 to 0.307. RMSE is root mean squared error, which penalizes larger misses more heavily; MAE is mean absolute error, the average absolute prediction miss.1
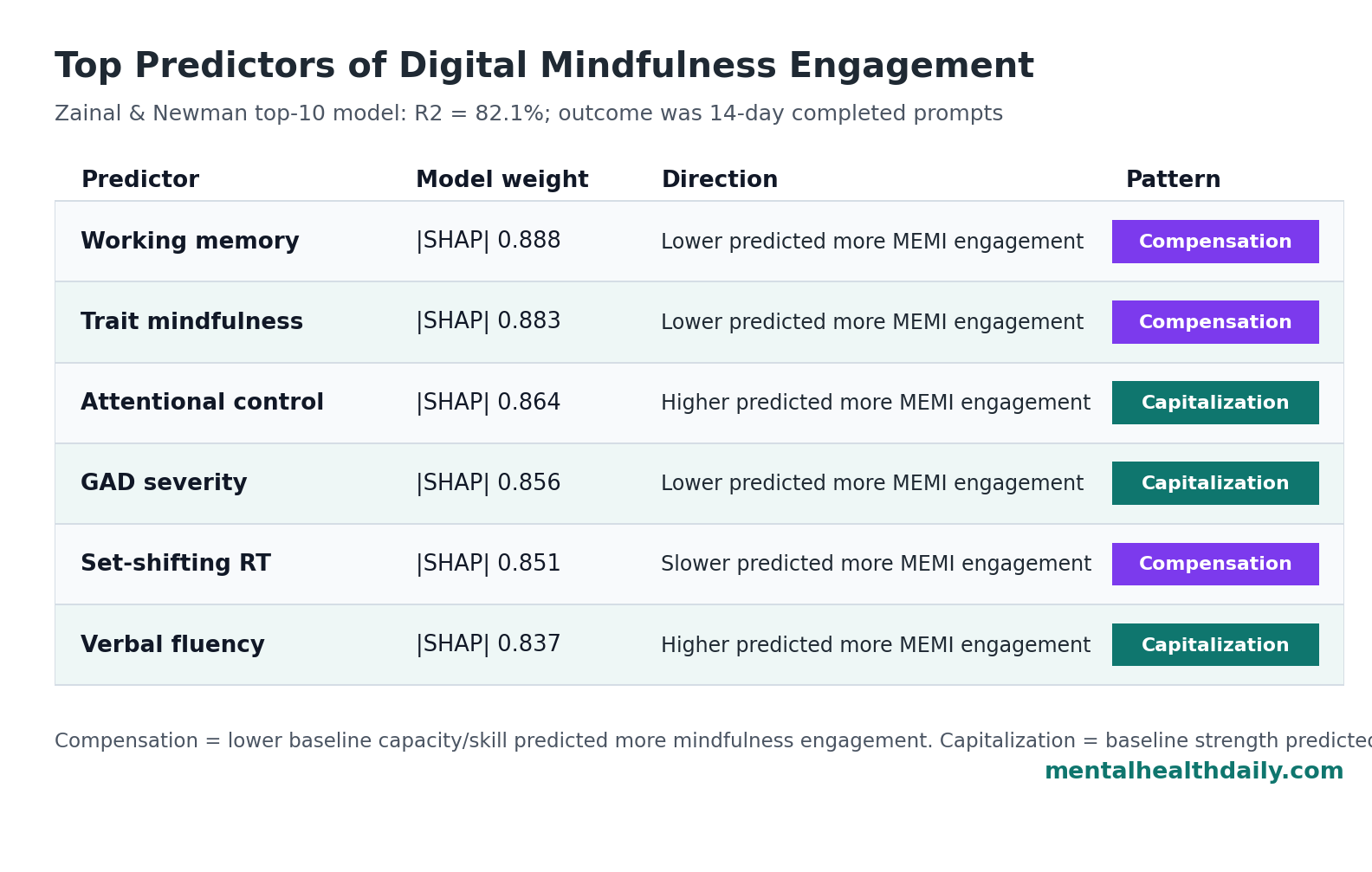
SHAP values are model-interpretation scores that estimate how much each predictor contributes to the model’s output after accounting for the other variables. Working memory ranked first with |SHAP| = 0.888, followed by trait mindfulness at 0.883, attentional control at 0.864, GAD severity at 0.856, set-shifting response time at 0.851, verbal fluency at 0.837, empathy and treatment expectancy at 0.829, inhibition at 0.818, and executive dysfunction at 0.816.1
Mindfulness Engagement Reflected Capitalization and Compensation
The result did not support a single “motivated and high-functioning users engage more” story. Some predictors fit a capitalization pattern, where people with useful baseline strengths engage more with the active intervention. Other predictors fit a compensation pattern, where people with a deficit engage more because the intervention supplies structure they lack.
- Capitalization signals: higher attentional control, higher verbal fluency, and higher empathy predicted more engagement with MEMI than with self-monitoring. These strengths plausibly help a person understand, remember, and apply brief mindfulness instructions across ordinary routines.1
- Compensation signals: lower working memory, lower trait mindfulness, lower treatment expectancy, and slower set-shifting response time also predicted more engagement with MEMI than with self-monitoring. MEMI may have supplied repeated scaffolding for people who lacked baseline mindfulness skill or cognitive ease.1
- Symptom-severity signal: lower GAD severity predicted greater MEMI engagement relative to self-monitoring, suggesting that severe worry may make brief skill practice harder even when anxiety is the treatment target.1
That mix is clinically useful because it resists lazy personalization. Digital mindfulness may not be best targeted only to people who already look mindful, organized, and highly expectant. Low baseline mindfulness and skepticism can still leave room for engagement if the intervention feels useful quickly enough.
Prior Digital-Mental-Health Evidence Makes Engagement Worth Studying
The 2026 analysis sits on top of a parent randomized trial that tested the same 14-day MEMI against self-monitoring in generalized anxiety disorder.2 A later model from the same research line asked a related but different question: who benefits symptomatically from MEMI vs. self-monitoring?3 The current article’s question was narrower and more operational: who actually completes the prompts?
That operational question is not trivial. A systematic review and meta-analysis by Gan et al. linked engagement with digital interventions to mental health outcomes, while a 117-trial meta-analysis by Zainal et al. treated digital mental health intervention engagement as a problem that varies by user, intervention, and study design.4,5
Prediction-model reviews in psychiatry add the caution. Meehan et al. found that clinical prediction models have become more common, but validation, transportability, and implementation remain recurring weak points.6 A small internally validated app-engagement model can be promising and still fall short of a treatment-selection rule.
Limitations of This Engagement Model
The design supports a research-level engagement signal, not an app-prescription calculator.
- Small sample: N = 110 is modest for machine learning. Nested cross-validation reduces optimism, and external replication remains necessary.
- Short duration: the model predicted 14-day prompt completion, not 6-month app use, maintenance practice, or relapse prevention.
- Single engagement metric: completed prompts do not capture whether participants practiced deeply, learned the skill, returned voluntarily, or improved clinically.
- Limited representativeness: the sample was mostly young, predominantly female, and predominantly White. Engagement rules may shift in older, more clinically severe, more racially diverse, or routine-care populations.
- Internal validation only: the top-10 predictor set needs testing in an independent sample before clinicians or app platforms should use it for matching.
The strongest use of this paper is therefore methodological and practical: digital mindfulness engagement can be modeled with more nuance than “users either comply or do not.” The weaker use would be treating R2 = 82.1% as proof that a deployment-ready matching algorithm exists.
Questions About Digital Mindfulness Engagement for GAD
Did this study show that digital mindfulness reduces generalized anxiety symptoms?
No. This 2026 analysis studied engagement with prompts, not symptom reduction. The parent randomized trial addressed symptom effects, while this analysis asked who completed more mindfulness vs. self-monitoring prompts.2
What does R2 = 82.1% mean here?
It means the top-10 predictor model explained about 82.1% of variance in the log-transformed engagement outcome inside this internally validated dataset. Performance in a new clinic, app platform, or demographic group could be substantially different.
Why would lower trait mindfulness predict more engagement with mindfulness prompts?
Lower baseline mindfulness may create more room for the intervention to feel novel and useful. A person who already practices mindfulness may have less new skill value to gain from 1 to 2 minute prompts, while a low-mindfulness participant may experience the prompts as practical scaffolding.
Should clinicians use this model to assign patients to digital mindfulness?
Not yet. The model needs external validation, broader sampling, and outcome-linked testing. For now, it is better read as a proof-of-concept for engagement matching than as a clinical decision tool.
What is the practical takeaway for digital anxiety tools?
Engagement design should account for both capacity and need. Strong attention and verbal fluency may help users engage, but structured prompts may also attract people with lower working memory, lower mindfulness, or lower initial expectancy when the intervention gives them a clear skill to try.
References
- Zainal NH, Newman MG. Who engages? Machine learning insights into digital mindfulness-based intervention for generalized anxiety disorder. Journal of Affective Disorders. 2026;399:120963. doi:10.1016/j.jad.2025.120963
- Zainal NH, Newman MG. A randomized controlled trial of a 14-day mindfulness ecological momentary intervention (MEMI) for generalized anxiety disorder. European Psychiatry. 2023;66(1):e12. doi:10.1192/j.eurpsy.2023.2
- Zainal NH, Newman MG. Which client with generalized anxiety disorder benefits from a mindfulness ecological momentary intervention versus a self-monitoring app? Developing a multivariable machine learning predictive model. Journal of Anxiety Disorders. 2024;102:102825. doi:10.1016/j.janxdis.2024.102825
- Gan DZQ, McGillivray L, Han J, Christensen H, Torok M. Effect of engagement with digital interventions on mental health outcomes: a systematic review and meta-analysis. Frontiers in Digital Health. 2021;3:764079. doi:10.3389/fdgth.2021.764079
- Zainal NH, Wang V, Garthwaite B, Curtiss JE. What factors are related to engagement with digital mental health interventions (DMHIs)? A meta-analysis of 117 trials. Health Psychology Review. 2025. doi:10.1080/17437199.2025.2547610
- Meehan AJ, Lewis SJ, Fazel S, Fusar-Poli P, Steyerberg EW, Stahl D, Danese A. Clinical prediction models in psychiatry: a systematic review of 2 decades of progress and challenges. Molecular Psychiatry. 2022;27(6):2700–2708. doi:10.1038/s41380-022-01528-4