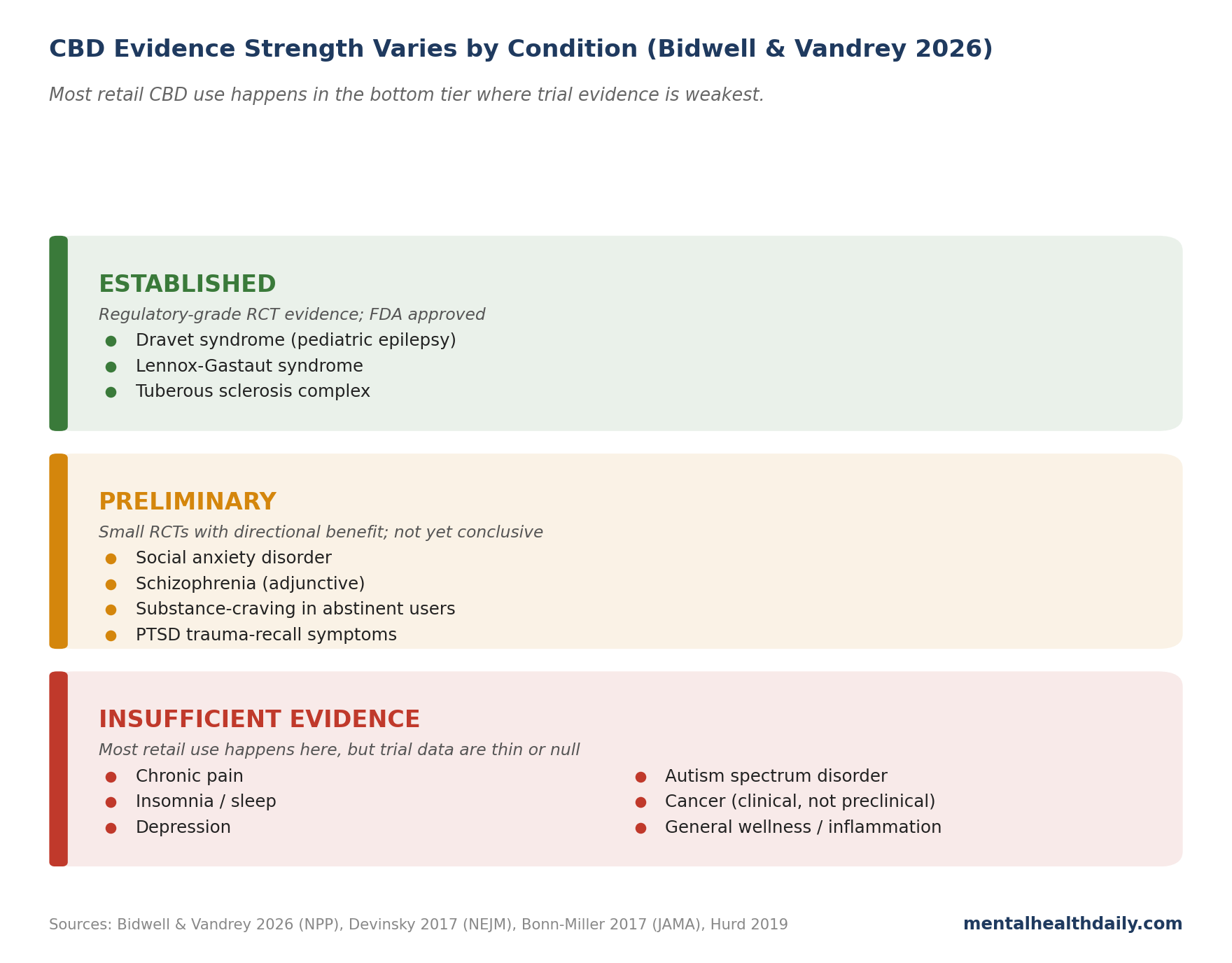
CBD went from a Schedule I controlled substance to a wellness category in less than a decade. The product label “CBD” now covers oils, gummies, topicals, vape liquids, beverages, beauty products, and pet treats — a $5 billion retail market in the US alone. Bidwell and Vandrey’s 2026 Circumspectives review in Neuropsychopharmacology takes the unusual step of presenting the optimistic and cautious cases side by side and then integrating them.1 The integrated read is the cleanest summary of where CBD evidence sits in 2026: a small, real signal in specific conditions, surrounded by a much larger product market that mostly isn’t supported by trial data.
Research Highlights
- The only well-established clinical use of CBD is rare pediatric epilepsy. Epidiolex, the FDA-approved purified CBD product, has solid trial evidence for Dravet syndrome, Lennox-Gastaut syndrome, and tuberous sclerosis complex. Outside these specific seizure disorders, the clinical evidence is much thinner.
- Anxiety and psychosis show real but preliminary signal. A handful of trials suggest CBD reduces social-anxiety symptoms and may have antipsychotic effects comparable to amisulpride for schizophrenia. The trials are small, short, and few — promising, not yet conclusive.
- Most retail CBD products are not what they claim. Surveillance studies show most CBD oils, edibles, and topicals are mislabeled — over half contain different amounts of CBD than the label states, and a significant minority contain detectable THC, pesticide residues, or heavy metals. Pharmaceutical-grade Epidiolex is a different product than what you find online or in dispensaries.
- CBD is not pharmacologically inert. It blocks CYP450 liver enzymes, which slows the metabolism of many other medications. At chronic high doses it can cause measurable liver-enzyme elevation. Co-use with other psychoactive medications is more complicated than the marketing suggests.
- The “CBD treats everything” framing has run far ahead of the evidence. Proven effective: rare epilepsies. Plausibly effective with thin trial data: social anxiety, schizophrenia adjunct, opioid-related craving, post-traumatic stress. Insufficient evidence: pain, sleep, depression, autism, PTSD broadly, cancer. The product you buy at a dispensary is likely a different formulation than the one tested in any of those trials.
Where the Evidence Is Strongest: Rare Pediatric Epilepsies
The only clinical condition where CBD has unambiguous, regulatory-grade evidence is rare drug-resistant epilepsies in children. Devinsky and colleagues’ 2017 pivotal trial in the New England Journal of Medicine tested purified CBD (Epidiolex, a pharmaceutical-grade isolate manufactured by Jazz Pharmaceuticals) against placebo in children with Dravet syndrome.2 The headline numbers:
- Convulsive seizure frequency dropped 39% on CBD vs. 13% on placebo — a meaningful and clinically significant difference. Treatment-responder rate (50% reduction in seizures) was 43% on CBD vs. 27% on placebo.
- Effects were seen on top of existing antiepileptic medications — the children stayed on their primary regimens, and CBD was added as adjunctive therapy. CBD didn’t replace standard treatment; it supplemented it.
- Adverse events were notable but manageable: somnolence, decreased appetite, diarrhea, and elevated liver enzymes (the latter mostly when co-administered with valproate).
Subsequent trials confirmed similar effects in Lennox-Gastaut syndrome and tuberous sclerosis complex. Epidiolex is now FDA-approved for these specific indications. This is the foundation of the entire “CBD has clinical effects” claim — and it is genuinely solid evidence for a narrow set of conditions.
Where the Signal Is Preliminary but Worth Watching: Anxiety, Psychosis, Substance Craving
Outside epilepsy, three psychiatric conditions have the strongest clinical signals, all from small trials.
Social anxiety disorder. Bergamaschi and colleagues’ 2011 trial gave CBD or placebo to 24 patients with social anxiety before a public-speaking task and measured anxiety, cognitive impairment, discomfort, and physiological arousal. CBD reduced subjective anxiety and the physiological response significantly compared to placebo.3 Subsequent small trials have replicated parts of this finding, but no large adequately-powered RCT in social anxiety disorder yet exists.
Schizophrenia. Leweke and colleagues’ 2012 trial compared CBD (800 mg/day) with amisulpride (a standard atypical antipsychotic) in 42 patients with acute schizophrenia.4 CBD was clinically comparable to amisulpride for symptom reduction over 4 weeks, with a meaningfully better side-effect profile (less weight gain, less prolactin elevation, less extrapyramidal symptoms). McGuire and colleagues’ 2018 RCT tested CBD as an adjunct to existing antipsychotics in 88 patients and found small but significant reductions in positive symptoms.5 The evidence is suggestive enough to warrant continued investigation, not yet sufficient to recommend CBD for schizophrenia in routine practice.
Substance use craving. Hurd and colleagues’ 2019 RCT in American Journal of Psychiatry gave CBD (400 or 800 mg) or placebo to 42 abstinent heroin users and showed CBD reduced drug-cue-induced craving and anxiety compared to placebo.6 The effect was modest, the trial was small, and the population was specific (abstinent, not actively using), but the direction is consistent with what the broader cannabinoid-system literature predicts.
The common pattern in all three: small N, short duration, single-site, mostly purified CBD at doses much higher than retail products typically deliver. Promising preliminary evidence, not yet at the level that would change clinical guidelines.
Where the Evidence Is Insufficient (Despite the Marketing)
Most of what CBD is sold for in the US has insufficient or mixed evidence. Black and colleagues’ 2019 systematic review of cannabinoids in psychiatric disorders made the same point at the broader cannabinoid level.8 The conditions consumers most commonly buy CBD for — pain, anxiety, sleep, depression — are exactly the conditions where the trial data are weakest.
Pain. A 2018 Cochrane review of cannabinoids for chronic neuropathic pain concluded the evidence was of low to very low quality and the magnitude of benefit was small.9 Most trials lumped CBD with THC; pure-CBD pain trials are rare and underpowered.
Sleep. CBD is widely marketed for sleep, but the trial data are sparse. Some short studies report small benefits at high doses; others find effects close to zero or attribute improvements to anxiolysis rather than direct hypnotic action. A 2023 review concluded the evidence base was insufficient to recommend CBD for insomnia.
Depression. Pure-CBD trials in depression don’t exist at adequate scale. Indirect evidence from anxiety reduction may translate to some mood benefit, but no RCT has tested CBD as a primary depression treatment in a meaningful way.
Autism. Small case series and observational reports suggest CBD may reduce irritability and self-injury in some children with autism, but no adequately powered RCT has been published. Bar-Lev Schleider’s 2019 observational study reported safety and tolerability but cannot establish efficacy.
Cancer. Preclinical models show antitumor effects in cell lines and animals; this has not translated to evidence of clinical benefit in humans. Bidwell and Vandrey explicitly flag the gap between preclinical signals and clinical evidence in oncology as a representative case of the broader CBD-evidence problem.
CBD Product Quality Problem
Even where the trial evidence is strong, the products available to consumers may not match what the trials tested. Bonn-Miller and colleagues’ 2017 surveillance study tested 84 CBD products purchased online and found:
- Only 31% were accurately labeled. 26% contained less CBD than claimed; 43% contained more.
- 21% contained detectable THC — some at concentrations that could produce intoxication or fail a drug test, despite being sold as THC-free.
- Vaporized products had the worst label accuracy; oils and tinctures were the most reliable category, though still mostly mislabeled.7
Subsequent surveillance work has continued to find similar problems. Pharmaceutical-grade Epidiolex (a purified CBD isolate manufactured to GMP standards under FDA oversight) is a fundamentally different product from a $40 bottle of “full-spectrum hemp oil” purchased at a gas station. Generalizing trial results from Epidiolex to retail CBD is not straightforward.
The Drug Interaction Problem
CBD is not pharmacologically benign. It is a potent inhibitor of multiple cytochrome P450 (CYP450) enzymes — the liver’s primary drug-metabolism pathway. Inhibiting these enzymes slows the breakdown of many co-administered medications, raising their blood levels and increasing adverse-effect risk. Two practical implications:
- Many psychiatric and neurological medications interact with CBD. Clobazam (an antiepileptic), warfarin (an anticoagulant), and various SSRIs and antipsychotics all show measurable interaction. Patients on these medications who add CBD may experience dose-equivalent increases in their primary medication’s effect — and sometimes adverse events.
- Chronic high-dose CBD can elevate liver enzymes. Most cases are managed with monitoring and dose adjustment, but the risk is documented across multiple datasets and shouldn’t be dismissed. The Epidiolex prescribing label includes a hepatic-monitoring recommendation; retail CBD products carry no comparable guidance.
The “CBD is safe and natural” framing in retail marketing is at odds with the pharmacology. CBD has a favorable safety profile relative to many psychiatric medications, but it is a real drug with real interactions, not a supplement.
CBD as a Medical Treatment in 2026: Evidence vs. Reality
The honest synthesis from the trial evidence:
- For Dravet, Lennox-Gastaut, or tuberous sclerosis complex with treatment-resistant seizures, prescription Epidiolex has solid evidence and is the appropriate path. This requires a neurologist, FDA-approved monitoring, and is reimbursable through health insurance.
- For social anxiety, schizophrenia, or substance-craving conditions, CBD is interesting but not yet first-line. The trial evidence is preliminary, and standard treatments (SSRIs for anxiety, atypical antipsychotics for schizophrenia, evidence-based addiction treatment for substance use) have stronger evidence and clearer regulatory paths.
- For pain, sleep, depression, autism, or general wellness, the evidence does not support CBD as effective treatment. Some users report benefits, but those benefits aren’t clearly distinguishable from placebo in the trial data, and product variability adds noise.
- If you decide to use a retail CBD product, accept that label accuracy is poor and the product may not match what trials studied. Look for third-party Certificate of Analysis (COA) testing from products that publish detailed lab results. Avoid products without independent verification.
- Always tell your prescriber about CBD use. The CYP450 interactions with common psychiatric and neurological medications are clinically meaningful, and your prescriber needs to know to monitor and adjust if necessary.
Common Questions About CBD
Does CBD work for anxiety?
For social anxiety specifically, small trials show reductions in self-reported anxiety and physiological arousal at doses of 300-600 mg.3 The evidence is preliminary and mostly involves pure CBD at doses higher than typical retail products deliver. For generalized anxiety, the evidence is even thinner. CBD is not yet first-line for anxiety; SSRIs and CBT have far stronger evidence.
Is CBD safe?
Generally yes at therapeutic doses, with two important caveats: chronic high doses can elevate liver enzymes, and CBD inhibits CYP450 liver enzymes, which slows metabolism of many other medications. If you take any prescription drug — especially anticoagulants, antiepileptics, or psychiatric medications — talk to your prescriber before starting CBD.
Why does my CBD product not work the way the studies suggest?
Three reasons. First, retail CBD products are often mislabeled — the dose stated on the bottle may not match what’s inside. Second, oral CBD has poor and variable bioavailability; you may absorb 5-15% of an oral dose. Third, trial doses are typically 200-800 mg/day, far higher than most retail products deliver per serving.7
Is full-spectrum better than isolate?
The “entourage effect” claim — that full-spectrum CBD with trace THC and minor cannabinoids works better than isolate — is theoretically reasonable but not strongly supported by trial data. Most rigorous trials use isolate; observational studies of full-spectrum users are confounded by selection bias. The pivotal Epidiolex trials all used purified isolate.
Can CBD show up on a drug test?
Yes, depending on the product. Many “THC-free” CBD products contain detectable THC at concentrations that can trigger positive results on standard workplace drug tests.7 If drug testing is a concern, use only products with current third-party certificates showing zero detectable THC.
Does CBD help with sleep?
The trial evidence is mixed and mostly weak. Some short studies report modest benefits at high doses; others find effects close to placebo. If CBD helps sleep, it may be by reducing pre-sleep anxiety rather than directly inducing sleep. CBT-I and standard sleep-medicine approaches have far stronger evidence for chronic insomnia.
References
- Cannabidiol at the crossroads: panacea, placebo, or problem? Bidwell LC, Vandrey R. Neuropsychopharmacology. 2026. doi:10.1038/s41386-026-02415-0
- Trial of cannabidiol for drug-resistant seizures in the Dravet syndrome. Devinsky O et al. New England Journal of Medicine. 2017;376(21):2011-2020. doi:10.1056/NEJMoa1611618
- Cannabidiol reduces the anxiety induced by simulated public speaking in treatment-naïve social phobia patients. Bergamaschi MM et al. Neuropsychopharmacology. 2011;36(6):1219-1226. doi:10.1038/npp.2011.6
- Cannabidiol enhances anandamide signaling and alleviates psychotic symptoms of schizophrenia. Leweke FM et al. Translational Psychiatry. 2012;2:e94. doi:10.1038/tp.2012.15
- Cannabidiol (CBD) as an adjunctive therapy in schizophrenia: a multicenter randomized controlled trial. McGuire P et al. American Journal of Psychiatry. 2018;175(3):225-231. doi:10.1176/appi.ajp.2017.17030325
- Cannabidiol for the reduction of cue-induced craving and anxiety in drug-abstinent individuals with heroin use disorder. Hurd YL et al. American Journal of Psychiatry. 2019;176(11):911-922. doi:10.1176/appi.ajp.2019.18101191
- Labeling accuracy of cannabidiol extracts sold online. Bonn-Miller MO et al. JAMA. 2017;318(17):1708-1709. doi:10.1001/jama.2017.11909
- Cannabinoids for the treatment of mental disorders and symptoms of mental disorders: a systematic review and meta-analysis. Black N et al. The Lancet Psychiatry. 2019;6(12):995-1010. doi:10.1016/S2215-0366(19)30401-8
- Cannabis-based medicines for chronic neuropathic pain in adults. Mücke M et al. Cochrane Database of Systematic Reviews. 2018;3:CD012182. doi:10.1002/14651858.CD012182.pub2