Research Highlights
- Wade 2026 (n = 11,036, ABCD Study) finds flattened cognitive trajectories in teen cannabis users, not absolute decline. Users started ahead at ages 9–10, then improved more slowly, falling behind controls by ages 15–17.1
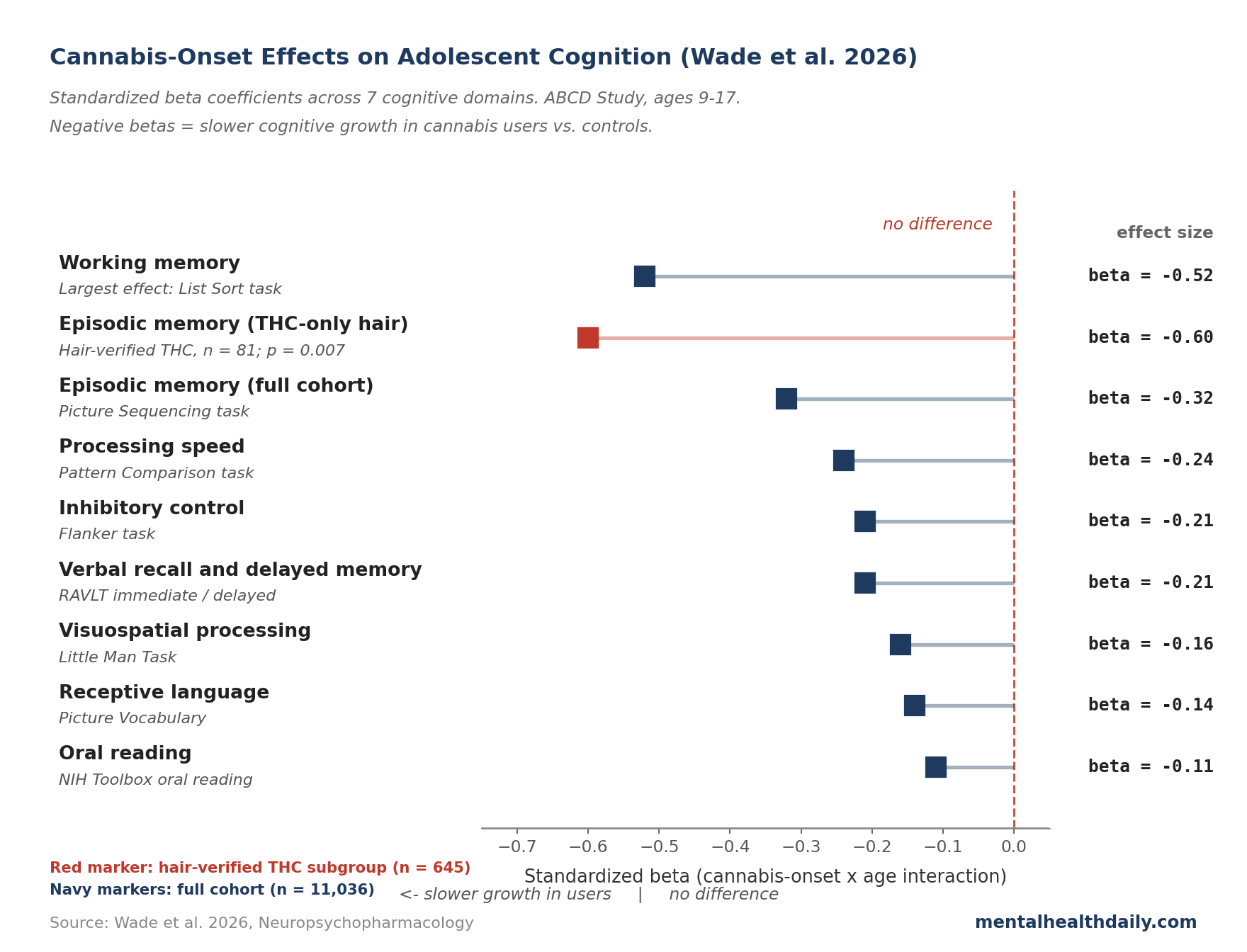
- Effects span 7 cognitive domains. Standardized β coefficients ran from −0.11 (oral reading) to −0.52 (working memory).1
- THC and CBD separate cleanly. In a hair-toxicology subsample (n = 645), THC-positive youth showed worse episodic memory growth (β = −0.60, p = 0.007). CBD-positive youth did not differ from controls.
- “Weed lowers IQ” oversimplifies the mechanism. Meier 2012 popularized that story; Rogeberg 2013 showed socioeconomic confounding could account for much of it. Wade 2026 lands in between: trajectory effects survive rigorous adjustment, and pre-existing differences before any exposure are also well-documented.
- Practical read: delaying onset past age 16 is supported by the data; “weed destroys teen brains” is not. Early regular THC exposure slows expected cognitive growth measurably — small to medium effects across most domains, larger for working and episodic memory in heavier users.
Headlines about teen cannabis use cycle between two failure modes: the alarmist “weed shrinks teen brains” frame anchored to Meier 2012’s 8-point IQ drop,2 and the dismissive “kids are fine” frame citing Rogeberg’s 2013 reanalysis showing the IQ effect was partly confounded by socioeconomic status.3
Wade et al.’s 2026 ABCD analysis is the most methodologically careful picture yet, and it lands between the poles. Cognitive effects in heavy adolescent users are well-documented — but the mechanism is closer to a slowed developmental trajectory than direct neurotoxic decline, and THC vs. CBD cleanly separates the signal.
Wade 2026: 11,036 ABCD Youth, β = −0.60 on Episodic Memory
Wade 2026 in Neuropsychopharmacology draws from ABCD — a 21-site US longitudinal cohort (longitudinal meaning the same kids tracked repeatedly over years) that recruited 11,000 youth at ages 9–10 and has followed them through age 17.1 What makes ABCD powerful is (a) baseline measurement before nearly any participant had touched cannabis, and (b) toxicological verification through hair, urine, breath, and oral-fluid testing — not just self-report.
The primary analysis used time-varying cannabis exposure: each participant counts as a control until any verified use is identified, then joins the cannabis-use group for later waves. Mixed-effects models tested whether cannabis-use status interacted with age — whether users and non-users improved on cognitive tests at different rates as they grew up. The interaction was significant across all 7 domains (FDR-corrected p < 0.05; FDR correction lowers the false-positive rate when many tests are run at once). Standardized β coefficients (effect sizes that put different tests on a common scale) ran from −0.11 for oral reading up to −0.52 for working memory.
The hair subsample is where the mechanism becomes legible. Among 645 youth with repeat hair testing at ages 12–16, those with THC detected (n = 81) showed substantially worse episodic memory growth: β = −0.60 (p = 0.007). CBD-positive youth (n = 21) did not differ from controls on any task. The CBD subgroup is too small for the null to establish CBD safety, but the THC-CBD divergence aligns with adult work showing the two cannabinoids have opposite cognitive profiles.4
Flattened Cognitive Trajectories, Not Absolute Decline
The most important nuance in Wade 2026 is the shape of the cognitive curves, not their endpoints. Cannabis users started ahead of controls at ages 9–10 across working memory, processing speed, inhibitory control, episodic memory, and language — before nearly any of them had used cannabis. Their scores still improved with age, just more slowly. By ages 15–17, the early advantage was gone or reversed across most domains. Working memory was the steepest: groups overlapped at ages 15–16 and users performed worse by age 17.
This is mechanically distinct from “cannabis lowers IQ” in the Meier 2012 sense, which described absolute IQ decline from childhood to midlife in persistent users.2 Wade 2026 participants are still adolescents and still improving. The data show reduced age-related growth, consistent with cannabis exposure during a sensitive neurodevelopmental window disrupting normal trajectory rather than poisoning the brain in any direct sense.5 Most users still scored within normal population ranges; “your kid won’t reach their cognitive potential” is more accurate than “your kid will be permanently impaired.”
Why Pre-Existing Differences Confound the Cannabis IQ-Drop Story (Meier 2012 vs. Rogeberg 2013)
Meier et al. 2012 reported an 8-point IQ drop from childhood to age 38 in persistent cannabis users in the Dunedin cohort, a New Zealand birth cohort followed since 1972.2 Coverage treated this as proof cannabis directly reduces intelligence. Rogeberg’s 2013 PNAS reanalysis complicated that read.3
In a simulated cohort matched on socioeconomic status (SES), some of the apparent IQ decline could be reproduced without any cannabis-induced damage — just from patterns of who uses cannabis heavily and how SES correlates with measured IQ change. The Meier finding pointed in the cannabis-harm direction but couldn’t rule out SES confounding.
Wade 2026 handles confounding more rigorously than any prior cohort — including parental education, family history of substance-use disorder, prenatal substance exposure, baseline psychopathology, race/ethnicity, sex, and other concurrent substance use, with an inverse propensity score absorbing leftover effects from things the covariate list can’t capture. Even so, the cannabis-onset × age interaction holds across 7 domains.
What the authors can’t rule out: shared vulnerability for both cannabis use and reduced cognitive growth (personality traits like openness, unmeasured family-environment factors), plus regression to the mean from elevated childhood baselines. The defensible read: documented cognitive differences in heavy adolescent users exceed what SES adjustment alone can explain. Whether THC exposure causes them, or shared vulnerability drives both heavier use and slower maturation, isn’t fully settled. The THC-specific hair finding tilts toward the first explanation without closing the case.
THC and CBD Separate Cleanly in the ABCD Data
Public conversation about “cannabis” lumps together products that are pharmacologically very different. THC (delta-9-tetrahydrocannabinol) is the primary psychoactive cannabinoid — it makes cannabis intoxicating and binds CB1 receptors heavily. CBD (cannabidiol) is non-intoxicating, modulates CB1 differently, and in some adult studies appears to blunt THC’s cognitive effects.4
Wade 2026’s hair subsample (samples reflect exposure over roughly 3 months) grouped youth: THC only (n = 81), CBD-positive (n = 21), controls (n = 546). The THC-only group showed worse episodic memory growth (β = −0.60, p = 0.007); at ages 15–17 they scored measurably worse than both controls and the CBD group on picture-sequencing. CBD-positive youth were indistinguishable from controls. Caveats: the CBD group is too small to establish safety; hair samples positive only for THC may include external contamination; and secondary analyses used p < 0.01 rather than FDR correction.
The THC-CBD divergence aligns with adult work. Morgan et al. 2012 showed adult users whose cannabis had higher CBD-to-THC ratios scored better on memory tests than THC-dominant users.4 Mokrysz et al. 2016 found acute THC produced larger memory deficits in adolescent males than adults.6 The compound matters — and the modern high-THC, low-CBD market is the worst of both worlds for the developing brain.
How Wade 2026 Fits Into Prior Literature
Scott et al.’s 2018 JAMA Psychiatry meta-analysis pooled 69 cross-sectional studies (n = 2,152 users, n = 6,575 controls).7 Pooled effects were small (d = −0.25) and shrank to negligible (d = −0.08) when analyses required 72+ hours of abstinence — suggesting much of the cross-sectional deficit may reflect lingering acute effects rather than persistent damage. Wade 2026’s longitudinal design complicates that read: if deficits were purely acute, they’d be constant over time, but the cannabis-control gap widens with age, more consistent with a developmental process than a steady-state recovery curve.
Volkow et al. 2014 in NEJM emphasized adolescent vulnerability through CB1-receptor density changes during pubertal neurodevelopment;8 imaging studies show small but reliable structural and functional differences in regular users, particularly in hippocampus and prefrontal cortex.9 Wade 2026 fits this picture: small to medium effects, larger for memory and executive function, mechanism plausibly tied to disrupted endocannabinoid signaling during a sensitive developmental window.
Limitations of ABCD’s Follow-Up Window
Adolescent users started ahead. The cannabis-use group out-performed controls at ages 9–10 across most tests. Some of the apparent decline at ages 15–17 reflects regression to the mean from elevated childhood baselines, not pure cannabis-induced decline.
Adult outcomes aren’t measured yet. ABCD currently runs through ages 17–18. Whether the flattened trajectories translate to durable adult deficits, or whether users catch up after cessation, won’t be known until the cohort is followed through their 30s.
Hair-toxicology subsample is small. The strongest mechanism evidence (THC-specific effect on episodic memory) comes from 81 THC-positive and 21 CBD-positive youth. The CBD null is consistent with safety but doesn’t establish it.
Unmeasured factors could still drive the link. Wade’s covariate set is comprehensive but not exhaustive. Personality traits like openness, peer-group factors, and undocumented adverse childhood experiences could plausibly drive both cannabis initiation and slowed cognitive growth without cannabis being the proximate cause.
Generalization to high-potency products is uncertain. ABCD recruitment began in 2016–2018. Commercial high-THC concentrates and edibles weren’t as ubiquitous as they are in 2026; the effects observed here may underestimate what current adolescent users experience with dispensary-grade THC.
What This Means for Parents and Teens
Early regular THC exposure during adolescence is associated with measurably slower cognitive growth across multiple domains, with effects proportional to exposure intensity. That’s meaningful but not “weed destroys your brain.” Most teen users in ABCD still scored within normal ranges; the gap is in growth rate.
- Delaying onset past age 16 is supported by the evidence. Multiple cohort studies show earlier onset predicts larger cognitive effects.11 The endocannabinoid system is still maturing through the late teens, and disruption during this window is harder to recover from than later exposure.
- Frequency matters more than ever-use. Hair toxicology only catches twice-monthly-or-more use, and that’s where the steepest effects concentrate. Occasional one-off experimentation isn’t where the cognitive risk lives.
- THC-dominant products are the cognitive risk; CBD products in this dataset weren’t. CBD products marketed for teen sleep or anxiety aren’t proven safe (the ABCD CBD sample was tiny), but they don’t show the THC signal. Mislabeling and contamination are documented — some commercial CBD products contain undisclosed THC.10
- The “weed makes you dumb” frame is wrong on mechanism but right on direction. The popular story misidentifies the effect as direct toxicity instead of disrupted development. Either way, the practical recommendation holds: delay onset, limit frequency if used, prefer lower-THC products.
Common Questions About Cannabis and the Teen Brain
Does cannabis lower IQ in teenagers?
Heavy adolescent-onset cannabis use is associated with slower cognitive growth across multiple domains. Whether this translates to a true adult IQ drop is less settled — Meier 2012 found an 8-point decline by age 38, but Rogeberg 2013 showed socioeconomic confounding could account for some of it.2,3 Wade 2026 finds smaller, broader effects during adolescence itself, more consistent with disrupted development than direct decline.1
Are CBD products safe for teens?
In Wade 2026, hair-CBD-positive youth (n = 21, no THC) showed no cognitive differences from controls — reassuring but underpowered. Two documented concerns remain: many commercial CBD products are mislabeled and contain undisclosed THC,10 and CBD’s long-term effects on adolescent neurodevelopment haven’t been studied carefully.
How much cannabis use causes cognitive effects?
Hair toxicology is sensitive to twice-monthly-or-more use, and the strongest effects in Wade 2026 came from this hair-verified subsample. Regular use is where the cognitive cost concentrates; occasional one-off use likely sits below detection and may carry smaller risk. No specific safe-frequency threshold is established.
If my teen already used cannabis, is the damage done?
No clean answer yet. ABCD only extends through ages 17–18, so post-cessation recovery in adolescent users hasn’t been studied longitudinally. Adult studies generally show partial cognitive recovery after sustained abstinence; Meier 2012 suggests persistent decline mainly in those who continued heavy use into adulthood. Stopping or reducing is plausibly beneficial; the magnitude of recovery isn’t pinned down.
Is medical cannabis okay for teens with anxiety or ADHD?
No high-quality evidence supports cannabis for adolescent anxiety, ADHD, or depression. Most trial data come from adults, and adolescent studies generally show worse outcomes in users with these conditions. A teen using cannabis to cope with anxiety is a signal to address the anxiety with evidence-based treatments, not to formalize the cannabis use.
References
- Longitudinal neurocognitive trajectories in a large cohort of youth who use cannabis: combining self-report and toxicology. Wade NE et al. Neuropsychopharmacology. 2026. doi:10.1038/s41386-026-02395-1
- Persistent cannabis users show neuropsychological decline from childhood to midlife. Meier MH et al. Proceedings of the National Academy of Sciences. 2012;109(40):E2657-E2664. doi:10.1073/pnas.1206820109
- Correlations between cannabis use and IQ change in the Dunedin cohort are consistent with confounding from socioeconomic status. Rogeberg O. Proceedings of the National Academy of Sciences. 2013;110(11):4251-4254. doi:10.1073/pnas.1215678110
- Sub-chronic impact of cannabinoids in street cannabis on cognition, psychotic-like symptoms and psychological well-being. Morgan CJA et al. Psychological Medicine. 2012;42(2):391-400. doi:10.1017/S0033291711001322
- Cannabis use and neurocognitive performance at 13-14 years-old: optimizing assessment with hair toxicology in the Adolescent Brain Cognitive Development (ABCD) study. Wade NE et al. Addictive Behaviors. 2024;150:107930. doi:10.1016/j.addbeh.2023.107930
- Are adolescents more vulnerable to the harmful effects of cannabis than adults? A placebo-controlled study in human males. Mokrysz C et al. Translational Psychiatry. 2016;6:e961. doi:10.1038/tp.2016.225
- Association of cannabis with cognitive functioning in adolescents and young adults: a systematic review and meta-analysis. Scott JC, Slomiak ST, Jones JD, Rosen AFG, Moore TM, Gur RC. JAMA Psychiatry. 2018;75(6):585-595. doi:10.1001/jamapsychiatry.2018.0335
- Adverse health effects of marijuana use. Volkow ND, Baler RD, Compton WM, Weiss SRB. New England Journal of Medicine. 2014;370(23):2219-2227. doi:10.1056/NEJMra1402309
- Mechanisms contributing to cognitive deficits in cannabis users. Mizrahi R, Watts JJ, Tseng KY. Neuropharmacology. 2017;124:84-88. doi:10.1016/j.neuropharm.2017.04.018
- Cannabidiol (CBD) product contamination: quantitative analysis of delta-9-tetrahydrocannabinol concentrations found in commercially available CBD products. Johnson E, Kilgore M, Babalonis S. Drug and Alcohol Dependence. 2022;237:109522. doi:10.1016/j.drugalcdep.2022.109522
- Dare to delay? The impacts of adolescent alcohol and marijuana use onset on cognition, brain structure, and function. Lisdahl KM, Gilbart ER, Wright NE, Shollenbarger S. Frontiers in Psychiatry. 2013;4:53. doi:10.3389/fpsyt.2013.00053