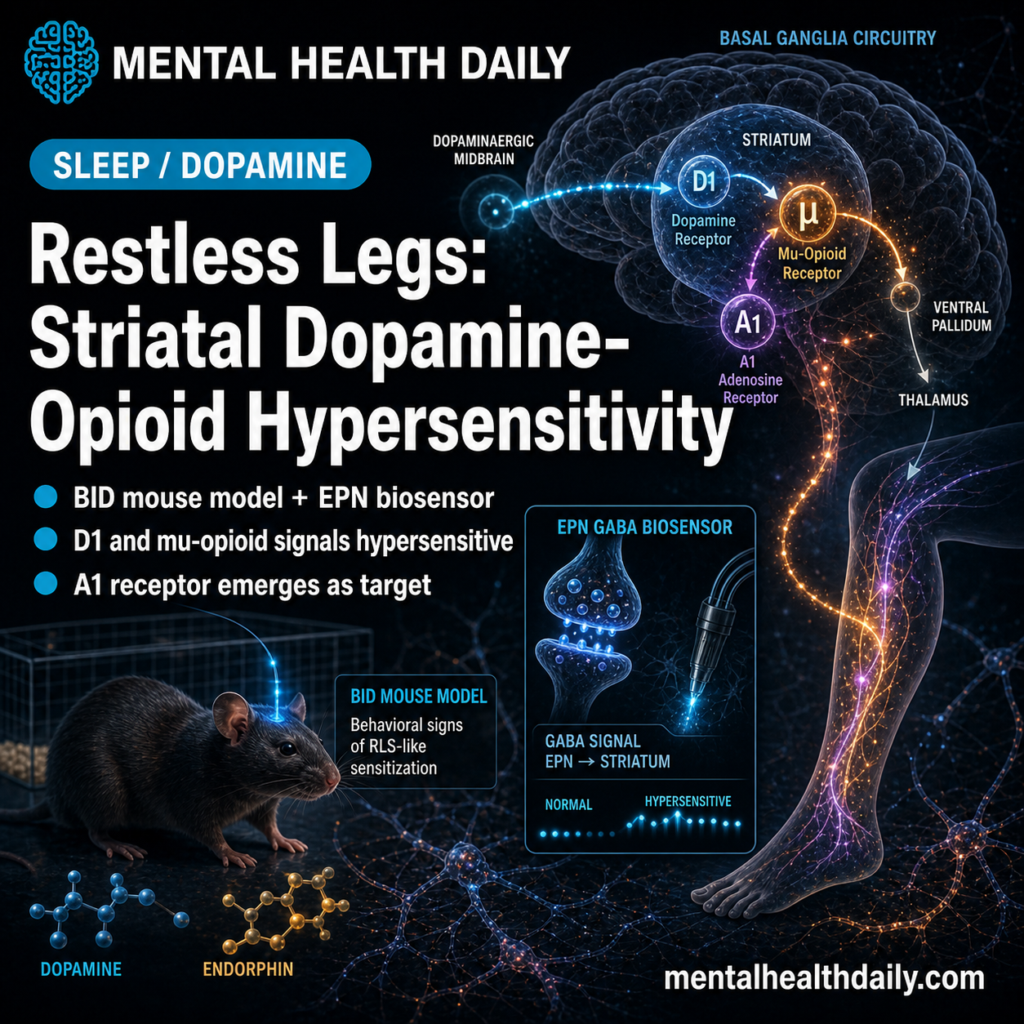
Restless legs syndrome (RLS) and opioid-withdrawal restlessness both produce night-worsening urges to move. A 2026 npj Parkinson’s Disease mouse study tied that overlap to hypersensitive striatal D1-mu-opioid receptor signaling in basal-ganglia motor circuits.1
Research Highlights
- 2 clinically similar states converged: restless legs syndrome and opioid-withdrawal restlessness both point toward a striatal D1-mu-opioid circuit that regulates motor output.1
- 1 iron-deficient mouse model localized the signal: viral GABA biosensing in the entopeduncular nucleus tracked output from the rodent equivalent of the human GPi.1
- 2 agonists exposed hypersensitivity: SKF81297 and methadone produced exaggerated D1-MOR pathway responses in brain-iron-deficient mice.1
- D1-MOR neurons became the treatment-relevant node: the same striosomal population helps explain dopamine-agonist benefit, opioid responsiveness, and augmentation risk.1
- A1 receptor biology adds a future target: striatal mRNA shifts implicated adenosine A1R signaling, but this remains an animal-model treatment hypothesis.1
Why the Clinical Overlap Suggested Shared Circuitry
Clinical overlap: RLS and opioid withdrawal restlessness both produce a deeply unpleasant urge to move that worsens with rest, peaks at night, and responds — sometimes dramatically — to opioids. Methadone, oxycodone, and tramadol are recognized RLS treatments for severe refractory cases despite the well-known risks. Shared opioid responsiveness was the first clue that the 2 conditions might converge on overlapping mechanisms.2
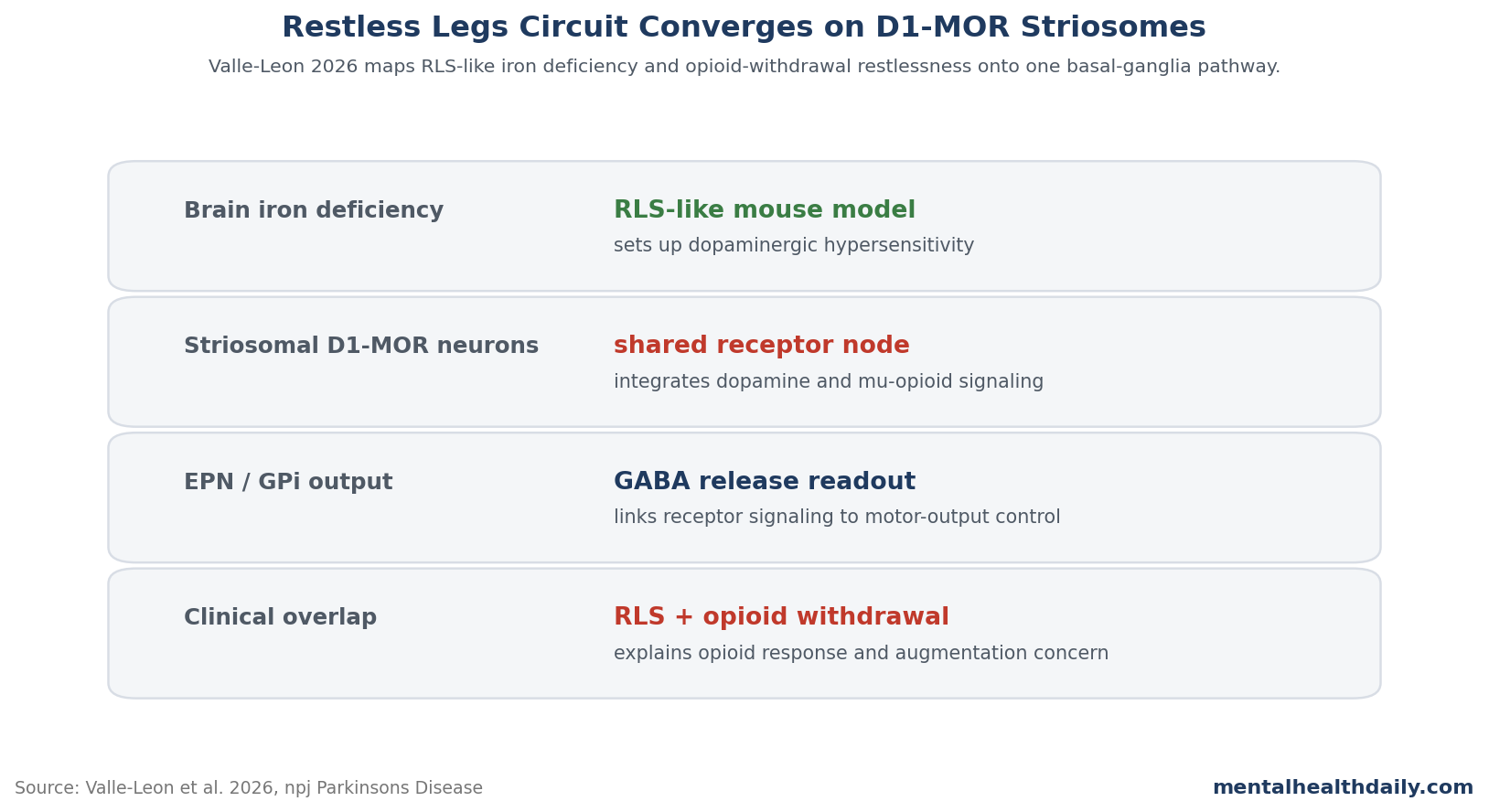
The researchers hypothesized that the convergence runs through striatal striosomal projection neurons that co-express D1 dopamine receptors and mu-opioid receptors and project GABAergic output to the GPi (rodent: entopeduncular nucleus, EPN). These neurons are part of the striatonigral “direct pathway” that disinhibits motor output through GPi inhibition.
If brain iron deficiency makes these neurons hypersensitive, both D1 activation (which the dopamine system normally provides) and mu-opioid activation (which exogenous opioids provide) should produce exaggerated behavioral effects. That’s exactly the pattern the experiments documented.1
What Brain-Iron-Deficient Mice Tell Us About RLS
The BID mouse model is built on a key insight from human RLS pathology: brain iron is consistently low in the substantia nigra and other regions in RLS, even when peripheral iron stores are adequate. Diet-induced brain iron deficiency in mice produces several RLS-relevant phenotypes including circadian-aligned hyperactivity and altered dopaminergic function.3
The model isn’t a perfect recapitulation of human RLS — mice don’t report the subjective sensory experience that defines clinical RLS — but it captures the iron-deficiency–dopaminergic-dysfunction–motor-restlessness chain that human research has implicated.
This experiment made the model testable at the level of specific receptor signaling. By injecting a viral GABA biosensor into the EPN and recording from awake mice during pharmacological challenge, the researchers could measure GABAergic output from the D1-MOR-co-expressing population.
Study snapshot: the decisive fiber-photometry experiment compared iron-deficient mice with control-diet mice after systemic SKF81297, a D1 receptor agonist. At 1.5 mg/kg, SKF81297 increased EPN GABA release in the iron-deficient group (n = 17) but not in controls (n = 12), showing that the same dopamine-receptor push had a larger downstream effect after brain iron deficiency.1
Methadone then tested the opioid side of the circuit. A 10 mg/kg dose reduced basal EPN GABA release and blocked the SKF81297-evoked GABA response in iron-deficient mice, while separate locomotor experiments showed that the movement response and the EPN GABA signal were not identical readouts. That split localizes the dopamine-opioid interaction to a striosomal projection pathway that can be measured independently of gross activity.1
The D1-MOR Co-Expression Story
Striatal projection neurons split broadly into two classes: D1-expressing “direct pathway” neurons that disinhibit motor output, and D2-expressing “indirect pathway” neurons that inhibit it. A subset of D1 neurons in striosomes also co-express mu-opioid receptors, creating a population that integrates both dopaminergic and opioid signals before sending GABAergic output to the GPi/EPN.1
In iron-deficient mice, this population becomes hypersensitive. A minimal locomotor-activating dose of the D1 agonist SKF81297 — one that produces little response in control mice — produces robust activation in BID mice. Methadone produces parallel changes in EPN GABA release. The mRNA expression analysis showed shifts in D1R, MOR, and adenosine A1R levels consistent with adaptive changes to chronic iron deficiency.
The expression data sharpen the pharmacology rather than replacing it. Brain iron deficiency was associated with lower striatal Oprm1 and Adora1 mRNA, the genes encoding mu-opioid receptors and adenosine A1 receptors. Because A1 receptors normally restrain D1 receptor signaling, reduced A1 tone gives the model a plausible route from iron deficiency to dopamine hypersensitivity without requiring a simple dopamine-deficiency explanation.1
This isn’t just “more receptors.” The functional implication is that the same dopaminergic input that produces normal motor output in control conditions produces exaggerated direct-pathway activation in iron-deficient conditions — a circuit-level explanation for why RLS patients experience the urge to move at lower thresholds than controls.
Connecting to Opioid Withdrawal
The opioid-withdrawal connection runs through the same circuit from a different angle. Chronic mu-opioid agonist exposure produces tolerance and adaptation in MOR-expressing neurons. Withdrawal removes the agonist tone, leaving the neurons in a state where their normal D1 input produces exaggerated direct-pathway output — functionally similar to the BID mouse hypersensitivity.1
Both conditions converge on a state where striosomal D1-MOR projection neurons drive excessive GABAergic output to the GPi. The clinical phenotype — restlessness with urge to move — reflects this shared circuit dysfunction.
The implication is bidirectional. RLS treatment with opioids works partly because it suppresses the hyperactive direct pathway. Opioid withdrawal mimics RLS partly because it produces the same kind of striatal disinhibition. The two conditions aren’t just clinically similar — they share circuitry that’s been precisely localized.
What This Predicts About RLS Treatment
Several treatment-relevant predictions follow from the circuit model. Iron repletion should reduce the underlying hypersensitivity, which aligns with clinical evidence that iron supplementation improves RLS symptoms. Dopamine agonists work because they modulate the hypersensitive direct pathway, but augmentation (the long-term worsening of RLS on dopamine agonists) may reflect accumulated changes in the same circuit.4
The most provocative prediction is that adenosine A1 receptor pharmacology may be a useful intervention angle. Prior work on A1R–D1R interactions on striatal neurons makes the mRNA changes in BID mice more than an incidental finding. Adenosine-targeting drugs aren’t currently used for RLS, but the mechanism makes them an interesting research target.
Clinical guardrail: refractory RLS should be treated as a threshold-sensitivity problem in a mixed dopamine-opioid-adenosine pathway, not as a simple dopamine-deficiency state. That framing explains why iron repletion, alpha-2-delta ligands, opioid rescue, and dopamine-agonist reduction can all make sense in different clinical situations when symptom timing, augmentation history, and ferritin status differ.
The Augmentation Problem in a New Light
Augmentation — the paradoxical worsening of RLS that develops in some patients on long-term dopamine agonist therapy — has been a major clinical problem for the field. The standard explanation has been receptor desensitization or downstream adaptation, but the precise mechanism has remained unclear.5
Mechanism implication: the Ferré circuit model suggests augmentation may reflect accumulated changes in the striosomal D1-MOR population that progressively worsen the underlying hypersensitivity. If this is right, switching agents within the dopamine agonist class does not address the underlying problem; reducing dopamine agonist exposure or substituting alternative mechanisms (alpha-2-delta ligands, opioids, iron repletion) is theoretically preferred.
Limits of the Animal Model
BID mice capture key elements of RLS pathophysiology but don’t reproduce the full human syndrome. The subjective sensory component — the “creepy-crawly” sensation that defines clinical RLS — isn’t accessible in mouse models. Circadian phase differences (mice are nocturnal) complicate the night-worsening pattern that defines human RLS.1
The fiber photometry technique measures bulk GABA release rather than single-cell activity, so the inference about D1-MOR co-expressing population specifically is built on selective viral targeting and pharmacological dissection rather than direct recording.
Evidence strength: this is a mechanistic animal study, not a human treatment trial. It can localize a plausible circuit and generate pharmacology predictions, but it cannot prove that adenosine-targeting drugs, opioid strategies, or dopamine-agonist changes improve human RLS outcomes.
Translation to human RLS treatment requires the assumption that mouse striosomal D1-MOR populations behave like their human counterparts. The genetic and circuit conservation is reasonable but not perfect.
Questions About RLS Mechanism
Why does RLS get worse at night?
Multiple factors contribute: dopaminergic activity has circadian variation, brain iron status fluctuates with circadian iron metabolism, and the absence of competing motor activity unmasks the urge-to-move signal that’s present but suppressed during the day.
Are RLS and Parkinson’s disease related?
Both involve striatal dopamine, but they’re distinct conditions. Parkinson’s involves nigrostriatal dopamine loss; RLS involves dysregulation that doesn’t produce the cell loss seen in Parkinson’s. There’s some clinical overlap but the underlying pathology differs.
Why do opioids work for RLS?
The mu-opioid receptor signaling on striatal striosomal projection neurons appears to suppress the hyperactive direct-pathway output that drives RLS symptoms. The mechanism is now more precisely understood than it was a decade ago.
What does this mean for new RLS treatments?
The circuit-level picture supports development of agents targeting the specific striatal striosomal population, including adenosine receptor modulators, alternative opioid receptor approaches, and combinations that address iron-deficiency-induced hypersensitivity directly.
References
- Valle-León M et al. Dopaminergic hypersensitivity of the opioid-responsive striatal-entopeduncular pathway in a rodent model of restless legs syndrome. npj Parkinsons Dis. 2026. doi:10.1038/s41386-026-02413-2
- Trenkwalder C et al. Prolonged release oxycodone-naloxone for treatment of severe restless legs syndrome. Lancet Neurol. 2013;12(12):1141-1150. doi:10.1016/S1474-4422(13)70239-4
- Connor JR et al. Iron and restless legs syndrome: treatment, genetics and pathophysiology. Sleep Med. 2017;31:61-70. doi:10.1016/j.sleep.2016.07.028
- Allen RP et al. Restless legs syndrome and Parkinson disease. Neurology. 2018;91(7):e757-e768. PubMed
- Garcia-Borreguero D, Williams AM. Dopaminergic augmentation of restless legs syndrome. Sleep Med Rev. 2010;14(5):339-346. doi:10.1016/j.smrv.2009.11.006