A 2026 study of 250 mothers of children with intellectual and developmental disabilities (IDDs) found that family burden was strongly tied to lower social support, lower family quality of life, and lower happiness. In the structural model, the burden-happiness link was explained by perceived support and family quality of life rather than a direct burden-to-happiness path.1
Research Highlights
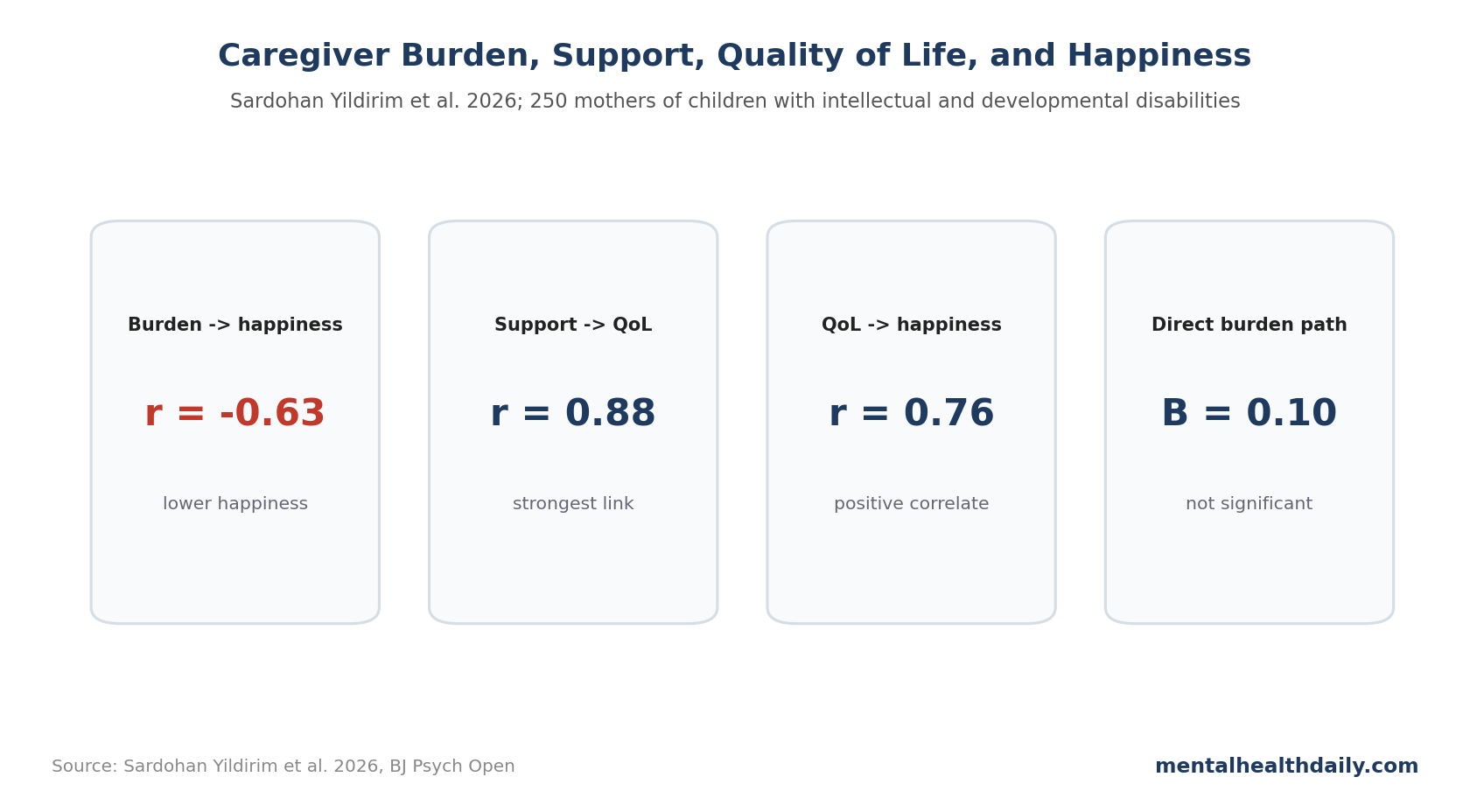
- Caregiver burden correlated with lower happiness: family burden and happiness were negatively correlated (r = −0.63, p < 0.001) in mothers of children with IDDs.1
- Social support was strongly connected to family quality of life: perceived social support correlated with family quality of life (r = 0.88, p < 0.001) and happiness (r = 0.72, p < 0.001).1
- Quality of life tracked happiness: family quality of life correlated with happiness (r = 0.76, p < 0.001), making it the most direct positive correlate in the model.1
- The direct burden path dropped out: when mediators were modeled, the direct family burden to happiness path was not significant (B = 0.10, p > 0.05).1
- Intervention target is specific: in this 250-mother sample, reducing caregiver burden may require strengthening usable support and family functioning instead of relying on generic resilience messages.
Caregiver burden is often described as an emotional state, but the construct is broader: time pressure, financial strain, administrative work, medical coordination, behavioral stress, family conflict, sleep loss, and worry about the child's future.
The mediation result changes the practical target. If support and family quality of life carry the burden-happiness relationship, the intervention target is the network and family system around the mother, not mood alone.
250 Mothers Completed Burden, Support, Quality-of-Life, and Happiness Measures
Sardohan Yildirim et al. studied 250 mothers of children with IDDs. The analysis used descriptive statistics, correlations, and structural equation modeling, a statistical method that estimates direct and indirect paths among latent constructs.1
The 4 core constructs were:
- Family burden: the practical and emotional load associated with caregiving.
- Perceived social support: whether help from family, friends, and significant others feels available and usable.
- Family quality of life: how well the family system is functioning across daily life, relationships, and needs.
- Happiness: subjective well-being measured with a short happiness scale.
The sample's mean family burden score was 162.26, perceived social support averaged 44.24, family quality of life averaged 66.13, and happiness averaged 17.97. Scale reliability was good: Cronbach's alpha was 0.93 for support, 0.98 for quality of life, 0.91 for burden, and 0.80 for happiness.1
Reliability affects the interpretation. If a scale is noisy, correlations can become unstable. Here, the internal consistency numbers suggest the constructs were measured coherently enough to take the pattern seriously.
Design limit: this was still a single-time caregiver survey. The model can show that burden, support, family quality of life, and happiness clustered in a coherent pathway, but it cannot prove which variable moved first. A family with better services may feel less burdened; a less overwhelmed mother may also be more able to seek support and keep routines stable.
Support and Quality of Life Were the Strongest Positive Correlates
The correlation matrix is the easiest part of the paper to understand. Burden moved in the opposite direction from the positive variables, while support and quality of life moved together.
- Support vs. family quality of life: r = 0.88, p < 0.001.
- Support vs. happiness: r = 0.72, p < 0.001.
- Support vs. family burden: r = −0.61, p < 0.001.
- Family quality of life vs. family burden: r = −0.68, p < 0.001.
- Family quality of life vs. happiness: r = 0.76, p < 0.001.
- Family burden vs. happiness: r = −0.63, p < 0.001.
Positive correlations mean the 2 variables rose together; negative correlations mean one was higher when the other was lower. In plain English, mothers reporting more support tended to report better family quality of life and greater happiness, while greater burden tended to travel with worse support, worse family quality of life, and lower happiness.
Structural Modeling Removed the Direct Burden-to-Happiness Path
The model first tested a partial mediation structure. In that version, the direct path from family burden to happiness was not statistically significant: B = 0.10, p > 0.05.1
The researchers then removed the direct path and tested full mediation. The final model showed acceptable fit: chi-square(99, N = 250) = 525.20, chi-square/df = 3.23, RMSEA = 0.061, SRMR = 0.061, TLI = 0.930, CFI = 0.942, NFI = 0.918, and IFI = 0.943.
For readers, those fit indices mean the model was not a random diagram drawn after the fact. It fit the observed covariance structure reasonably well for a social-science structural equation model, though it still does not prove causality.
The indirect effects were the main result:
- Burden through perceived support: B = −0.82, 95% BCa CI −1.18 to −0.55.
- Burden through family quality of life: B = −0.68, 95% BCa CI −0.91 to −0.47.
- Sequential support-to-quality-of-life pathway: B = −0.059, 95% BCa CI −0.113 to −0.085.
BCa CI means bias-corrected and accelerated confidence interval, a bootstrap interval used for indirect effects. If the interval does not cross zero, the mediation path is statistically supported.
Perceived Support Has to Be Usable Support
The study measured perceived social support rather than the number of relatives or friends around a family. A mother can have many people nearby and still feel alone if the help is judgmental, unreliable, poorly timed, or irrelevant to the actual daily burden.
In families of children with IDDs, usable support can include:
- Respite care: reliable time away from caregiving duties.
- Administrative help: support with appointments, school services, paperwork, transportation, and benefits.
- Emotional support: someone who can listen without minimizing the caregiving load.
- Peer support: other caregivers who understand disability-specific problems without requiring long explanation.
- Professional coordination: clinicians, therapists, educators, and social services communicating rather than fragmenting responsibility.
Service design needs this concrete level. “More support” is too vague to build around; useful support has to reduce actual friction in the mother's life.
Family Quality of Life Is the Larger Unit of Care
Family quality of life is not the same as the child's symptom severity or the mother's stress score. It asks whether family routines, relationships, resources, and daily functioning are sustainable.
The study's model points to a concrete care target. If family burden lowers happiness through family quality of life, then the care plan should not stop at measuring the child's disability or the parent's distress. It should ask what would make the household work better.
That can include sleep, sibling strain, transportation, school conflict, behavioral crises, financial pressure, marital strain, employment constraints, stigma, and lack of adult services as the child ages.
Those domains are also where a social-support score becomes clinically meaningful. A high perceived-support score should imply that someone can help during a behavior crisis, watch siblings during appointments, translate service rules, or reduce paperwork load. Otherwise, “support” risks becoming a pleasant but nonfunctional construct.
For families of children with IDDs, the burden source is rarely one isolated problem. The same week can include school meetings, therapy logistics, sleep disruption, behavior planning, medical appointments, and financial decisions. A family-quality-of-life lens is useful because it treats those problems as a connected household system rather than separate inconveniences.
Adjacent research in autism and IDD caregiving has repeatedly linked family hardiness, self-efficacy, support, and quality of life with caregiver outcomes.2,3 The Sardohan Yildirim analysis adds a clean model showing why those constructs should not be treated as soft extras.
Limitations of This Caregiver Burden Analysis
- Cross-sectional data: the model cannot prove that burden caused lower support or quality of life. Direction could be reciprocal.
- Mother-only sample: fathers, grandparents, siblings, and other caregivers may have different patterns.
- IDD heterogeneity: intellectual disability, autism, Down syndrome, and other developmental conditions can produce different caregiving demands.
- Self-report measures: common method bias can inflate correlations when all variables come from the same respondent.
- Context matters: support structures in Turkey may not map cleanly onto countries with different disability services, extended-family roles, or public benefits.
Questions About Caregiver Burden and Happiness
Does the study say caregiver burden does not affect happiness?
No. Burden correlated strongly with lower happiness. The model suggests the effect operated through perceived support and family quality of life rather than a direct path.
What does mediation mean here?
It means the statistical link between burden and happiness was explained by intermediate variables. Higher burden was tied to lower support and lower family quality of life, which were tied to lower happiness.
Is social support enough by itself?
Probably not. The study points to support and family quality of life together. A supportive text message is not equivalent to respite care, school coordination, financial help, or a workable daily routine.
What should caregiver-support programs change after this mediation result?
Caregiver interventions should target the family system along with the mother's coping style. Better practical support and better family quality of life are likely closer to the mechanism than generic resilience messaging.
References
- Family burden and happiness in mothers of children with intellectual and developmental disabilities: role of support and quality of life. Sardohan Yildirim AE, et al. BJ Psych Open. 2026. doi:10.1192/bjo.2026.11035
- Family hardiness, social support, and self-efficacy in mothers of individuals with autism spectrum disorders. Weiss JA, et al. Research in Autism Spectrum Disorders. 2013;7:1310-1317. doi:10.1016/j.rasd.2013.07.016
- Family quality of life among families with mild intellectual disability and mild autism spectrum disorder. Borilli MC, et al. Arquivos de Neuro-Psiquiatria. 2022;80:360-367. doi:10.1590/0004-282X-ANP-2020-0537
- Assessing family outcomes: psychometric evaluation of the Beach Center Family Quality of Life Scale. Hoffman L, et al. Journal of Marriage and Family. 2006;68:1069-1083. doi:10.1111/j.1741-3737.2006.00314.x
- The multidimensional scale of perceived social support. Zimet GD, et al. Journal of Personality Assessment. 1988;52:30-41. doi:10.1207/s15327752jpa5201_2