A 2022 Nature Communications study used non-contrast 3D T2-FLAIR magnetic resonance imaging (MRI) to map human brain lymphatic signals in living people, including apparent channels from cranial nerves and skull-base structures toward cervical lymph nodes.
Research Highlights
- Non-contrast MRI visualized lymphatic-like brain drainage: Albayram et al. identified dorsal dural signals near venous sinuses and ventral signals around cranial-nerve/skull-base routes in 81 people, without intravenous or intrathecal gadolinium.1
- Age changed the drainage pattern: participants older than 50 had thicker dorsal and ventral lymphatic signals, lower signal-intensity/thickness ratios, higher cerebrospinal fluid volume, and smaller cervical lymph-node measures.
- Dorsal and ventral systems moved together: overall dorsal and ventral thickness correlated (r = 0.45; p < 0.001), and the correlation remained after adjustment for age, sex, and intracranial volume (partial r = 0.32; p = 0.04).
- Neurodegeneration links remain indirect: animal and human studies connect meningeal lymphatics to aging, Alzheimer’s disease, Parkinson’s disease, and traumatic brain injury, but this MRI study did not test cognition or disease progression directly.26
- The main contribution is methodological: this 81-person MRI paper strengthens the case that human brain clearance can be studied in vivo, but it does not prove that enhancing lymphatic drainage treats dementia.
Human brain-clearance research has moved beyond arachnoid granulations as the only major drainage route. Newer work added meningeal lymphatic vessels, perineural routes along cranial nerves, and the glymphatic system, a CSF-interstitial-fluid exchange pathway proposed to help remove waste from brain tissue.
For mental health and neurodegeneration, the temptation is to jump straight from “brain drainage exists” to “brain drainage failure causes disease.” The better reading is slower: the anatomy is becoming visible, aging seems to change it, and disease hypotheses now have a plausible measurement target.
81 People Had Dorsal and Ventral Brain Lymphatic Signals on 3D FLAIR
Albayram et al. reviewed clinical MRI scans from people imaged for epilepsy or suspected epilepsy, then excluded scans with contrast exposure before the 3D FLAIR sequence, major motion artifact, surgery, stroke, mass lesions, status epilepticus, focal lesions, or other changes likely to distort normal drainage anatomy.
Study snapshot:
- Starting pool: 236 epilepsy-protocol MRI cases over 13 months.
- Final sample: 81 people, including 45 females and 36 males.
- Age range: mean 41.7 years (SD 20.4), range 15-80.
- Imaging method: 3-Tesla 3D T2-FLAIR MRI, 0.9-mm isotropic sections, no gadolinium contrast for the analyzed sequence.
- Main measurement: signal intensity and thickness of putative lymphatic structures in dorsal dural and ventral skull-base regions.
The method used intrinsic signal rather than injected tracer. In phantom testing, the parasagittal dural lymphatic signal corresponded to high albumin concentrations, roughly 2000-4000 mg/dL under the tested sequence parameters. The researchers argued that this made protein-rich lymphatic fluid and lymphatic tissue visible while suppressing ordinary CSF, vessels, white matter, muscle, bone, and fat.
Signals Tracked Venous Sinuses, Cranial Nerves, and Cervical Nodes
The dorsal system appeared near the superior sagittal sinus, straight sinus, confluence, transverse/sigmoid sinus regions, jugular veins, and posterior foramen magnum. The ventral system appeared around the anterior cranial fossa, olfactory region, optic groove, Meckel’s cave, internal auditory canal, and jugular foramen.
Visibility was not uniform. Some dorsal structures appeared in every scan, while others were seen in only a subset:
- Always visible: anterior/middle sagittal sinus drainage, straight sinus, confluence, left sigmoid-transverse junction, and posterior foramen magnum.
- Often but not always visible: posterior sagittal sinus in 59 of 81, transverse sinus in 57 of 81, right sigmoid sinus in 63 of 81, left sigmoid sinus in 61 of 81, left jugular vein in 47 of 81, and right jugular vein in 32 of 81.
- Ventral system: all measured ventral components were visible in all subjects, although the researchers warned that smaller structures may sit below the 0.9-mm resolution limit.
The dorsal and ventral systems were related, not random bright spots. Overall median dorsal and ventral thickness correlated (r = 0.45; p < 0.001), and still correlated after age, sex, and intracranial volume adjustment (partial r = 0.32; p = 0.04). Overall dorsal and ventral signal intensity also correlated (r = 0.49; p < 0.001; adjusted partial r = 0.55; p < 0.001).
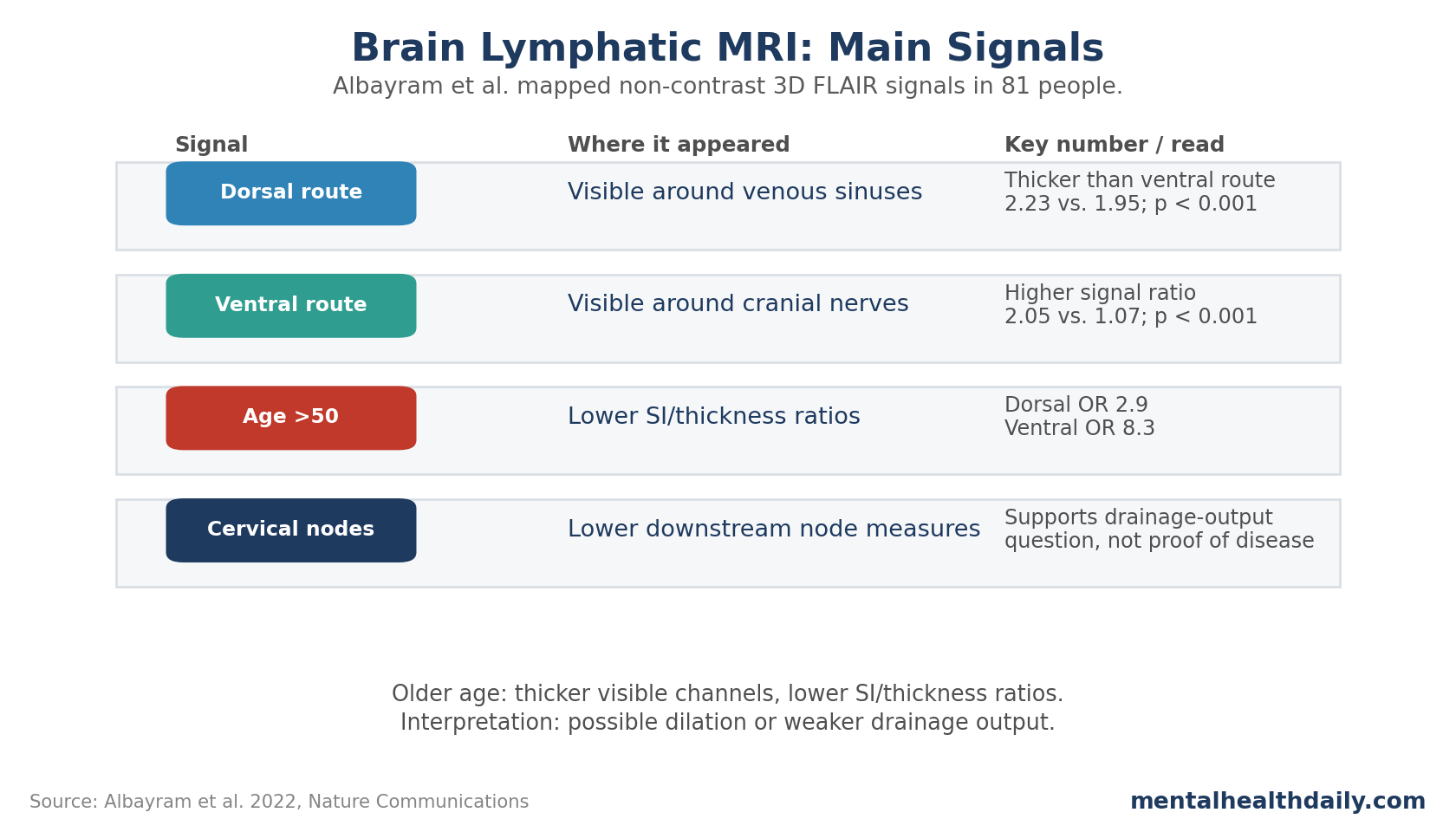
The ventral system had higher signal intensity relative to white matter than the dorsal system (2.05 vs. 1.07; p < 0.001). The dorsal system was thicker overall than the ventral system (median 2.23 vs. 1.95; p < 0.001). That paired pattern matters: stronger signal and greater thickness are not the same biological feature.
Older Age Was Linked to Thicker Channels and Smaller Neck Nodes
The age analysis was the piece most relevant to neurodegenerative speculation. A cutoff above 50 years discriminated lower vs. higher signal-intensity/thickness ratios with modest performance: area under the curve 0.68 for dorsal ratios (95% CI 0.56-0.79; p = 0.007) and 0.73 for ventral ratios (95% CI 0.62-0.85; p < 0.001).
In adjusted binary regression, age older than 50 was associated with lower dorsal and ventral signal-intensity/thickness ratios:
- Dorsal ratio: OR 2.9 (95% CI 1.1-7.7; p = 0.029).
- Ventral ratio: OR 8.3 (95% CI 2.8-24.7; p < 0.001).
- Age groups: 29 participants were older than 50, while 52 were younger than 50.
Older participants also had brain-volume patterns expected with aging: lower gray matter volume (647.9 vs. 712.0 cm3; p = 0.001), lower white matter volume (484.6 vs. 542.8 cm3; p = 0.017), and higher CSF volume (252.5 vs. 136.1 cm3; p < 0.001). Age correlated strongly with CSF volume (r = 0.75; p < 0.001), negatively with gray matter (r = −0.48; p < 0.001), and negatively with white matter (r = −0.34; p = 0.002).
The researchers interpreted thicker channels plus lower signal-intensity/thickness ratios as possible lymphatic dilation and reduced contractile function. Cervical lymph-node signal and short-axis measurements were also lower in older participants, so the age pattern favored a drainage-output problem over a simple bigger-is-better story.
Brain Lymphatic MRI Remains a Clearance Marker, Not a Dementia Treatment
The adjacent literature makes the result interesting. Aspelund et al. and Louveau et al. re-established meningeal lymphatic vessels in animal models in 2015, showing that the central nervous system had more conventional immune-drainage anatomy than older teaching allowed.23 Absinta et al. then showed that human and nonhuman primate meninges harbor lymphatic vessels visible by MRI, using contrast-enhanced imaging.4
Other human work strengthened the cervical-node link. Eide et al. reported MRI evidence of glymphatic drainage from the human brain to cervical lymph nodes.5 Zhou et al. reported impairment of the glymphatic pathway and putative meningeal lymphatic vessels in aging humans.6 In Parkinson’s disease, Ding et al. reported impaired meningeal lymphatic drainage in patients with idiopathic Parkinson’s disease.7
That does not make brain lymphatic dysfunction a master explanation for dementia. Alzheimer’s disease involves amyloid, tau, vascular injury, immune signaling, synaptic loss, sleep, genetics, and many other systems. The lymphatic angle is one route by which waste clearance, inflammation, and immune surveillance may intersect with those processes.
Limitations of This Brain Lymphatic MRI Study
The sample was clinical, not healthy-population sampling. Participants came from epilepsy or suspected-epilepsy imaging protocols. The authors excluded major structural confounds, but chronic seizure biology could still affect glymphatic or lymphatic signals.
The method inferred lymphatics from MRI signal. The study did not pair MRI findings with histology in the same living subjects. Hyperintense FLAIR signals in plausible locations are informative, but they remain imaging markers without same-subject microscopic proof.
Spatial resolution was limited. The 0.9-mm voxel size is strong for clinical MRI but coarse relative to tiny lymphatic structures. Smaller channels could be missed or blurred with adjacent tissues.
One neuroradiologist performed the image evaluation. Intra-rater reliability was excellent (ICC 0.983-1 for signal intensity and 0.995-1 for thickness; p < 0.001), but independent multi-rater replication would strengthen confidence.
Questions About Brain Lymphatic MRI
Does this study prove that poor brain drainage causes dementia?
No. It showed an imaging method and age-linked anatomical patterns. It did not measure dementia onset, cognitive decline, amyloid clearance, tau progression, or treatment response.
Why avoid gadolinium if contrast MRI can show lymphatic structures?
Gadolinium can be useful, but it is not ideal for repeated research in healthy or vulnerable populations. A non-contrast approach would make longitudinal studies safer and easier if the signal proves reliable.
What is the strongest practical implication?
Human brain clearance pathways can now be studied more directly. The next step is not a supplement or device claim; it is replication in healthy cohorts, Alzheimer’s disease, Parkinson’s disease, traumatic brain injury, sleep disorders, and vascular-risk groups.
For now, the result is best read as an imaging-method paper with aging biology attached.
Brain lymphatic MRI is not a finished biomarker yet. It gives aging and neurodegenerative disease researchers a measurable drainage pathway to test in longitudinal cohorts, disease samples, and intervention studies.
References
- Non-invasive MR imaging of human brain lymphatic networks with connections to cervical lymph nodes. Albayram MS et al. Nature Communications. 2022;13:203. doi:10.1038/s41467-021-27887-0
- A dural lymphatic vascular system that drains brain interstitial fluid and macromolecules. Aspelund A et al. Journal of Experimental Medicine. 2015;212(7):991-999. doi:10.1084/jem.20142290
- Structural and functional features of central nervous system lymphatic vessels. Louveau A et al. Nature. 2015;523:337-341. doi:10.1038/nature14432
- Human and nonhuman primate meninges harbor lymphatic vessels that can be visualized noninvasively by MRI. Absinta M et al. eLife. 2017;6:e29738. doi:10.7554/eLife.29738
- Magnetic resonance imaging provides evidence of glymphatic drainage from human brain to cervical lymph nodes. Eide PK et al. Scientific Reports. 2018;8:7194. doi:10.1038/s41598-018-25666-4
- Impairment of the Glymphatic Pathway and Putative Meningeal Lymphatic Vessels in the Aging Human. Zhou Y et al. Annals of Neurology. 2020;87(3):357-369. doi:10.1002/ana.25670
- Impaired meningeal lymphatic drainage in patients with idiopathic Parkinson’s disease. Ding XB et al. Nature Medicine. 2021;27:411-418. doi:10.1038/s41591-020-01198-1