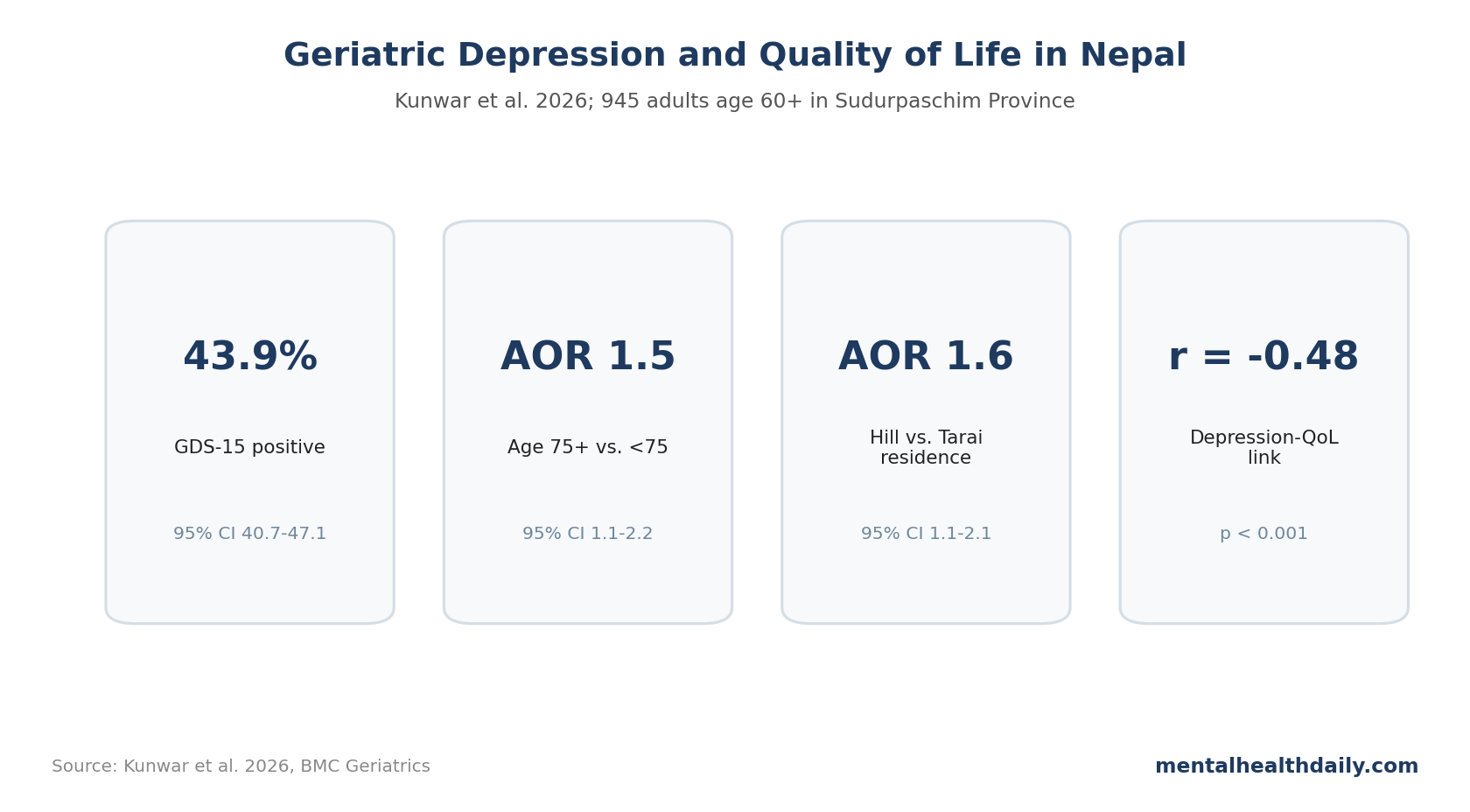
A 2026 community survey of 945 older adults in Nepal's Far-Western Sudurpaschim Province found geriatric depression in 43.9% of participants and a strong inverse link between depression scores and quality of life. The clearest adjusted predictors were age 75 or older and hill-region residence, while income and sex weakened after multivariable adjustment.1
Research Highlights
- Depression prevalence was high: Kunwar et al. reported geriatric depression in 43.9% of 945 community-dwelling adults age 60 and older in Sudurpaschim Province.1
- Age and geography survived adjustment: age ≥75 years had AOR = 1.5, 95% CI 1.1-2.2, and hill-region habitation had AOR = 1.6, 95% CI 1.1-2.1.1
- Quality of life moved with depression: total Geriatric Depression Scale score correlated with lower total WHOQOL-8 quality-of-life score (r = −0.48, p < 0.001).1
- Income looked important before adjustment: monthly income ≤20,000 Nepalese rupees had crude OR 2.1, but adjusted OR 0.9 after the full covariate model.1
- Screening needs context: a 15-item GDS cutoff can identify probable depression, but the practical response has to include health access, isolation, chronic disease, and local service pathways.
Geriatric depression refers to depressive symptoms in older adults, often intertwined with disability, bereavement, chronic illness, economic dependence, cognitive concern, sleep disruption, pain, and social shrinking.
The Nepal data are useful because the study measured quality of life, tested demographic and health correlates, and separated crude from adjusted associations alongside prevalence.
945 Older Adults Were Screened With GDS-15 and WHOQOL-8
Kunwar et al. selected 956 older adults, excluded 11 because of non-consent, hearing impairment, or unavailability, and analyzed 945 participants. The participation proportion was 98.8%, which is unusually strong for a community survey.1
The sample was almost evenly split by sex: 474 men and 471 women. Most participants were younger than 75 (77.9%), while 22.1% were age 75 or older. Hill-region residents made up 47.5%, and Tarai-region residents made up 52.5%.
The study used 2 short instruments:
- GDS-15: the 15-item Geriatric Depression Scale, a short depression screener designed for older adults. The Nepal study used a cutoff of 6 or higher for probable depression.
- WHOQOL-8: the 8-item World Health Organization quality-of-life index, covering subjective, physical, psychosocial, and environmental facets.
Short tools are a tradeoff. They make field work possible in older adults across rural and urban settings, but they do not replace diagnostic interviews. A GDS-15 positive result should be read as probable depressive symptom burden, not as a fully adjudicated psychiatric diagnosis.
43.9% Depression Prevalence Is the Main Signal
The prevalence estimate was direct: 43.9% of participants screened positive for geriatric depression, with 95% CI 40.7-47.1. Mean total GDS score was 5.3 with SD 3.1.1
Several subgroup percentages were higher than the overall sample:
- Age ≥75 years: 53.6% screened positive.
- Hill-region residence: 56.3% screened positive.
- Monthly income ≤20,000 NPR: 46.2% screened positive.
- Comorbid medical conditions: 48.4% screened positive.
Those percentages are useful for triage, but the adjusted model matters more. A subgroup can look high because it is older, poorer, sicker, geographically different, or some combination of those.
After adjustment, the study's durable demographic signals narrowed to age and hill-region residence. The adjusted model concentrated the independent signal around age and geography. Poverty and sex may still matter in other datasets, but this particular model did not keep them statistically significant after covariate adjustment.
Age 75+ and Hill Residence Stayed Significant After Adjustment
The crude model suggested several associations. Older age, female sex, hill residence, lower income, non-smoking, no alcohol use, and comorbid medical conditions each showed bivariate links with depression.1
The multivariable model narrowed the set:
- Age ≥75 years: AOR = 1.5, 95% CI 1.1-2.2, p = 0.019.
- Hill-region residence: AOR = 1.6, 95% CI 1.1-2.1, p = 0.006.
- Female sex: AOR 1.2, 95% CI 0.8-1.7, p = 0.24.
- Income ≤20,000 NPR: AOR 0.9, 95% CI 0.6-1.5, p = 0.94.
- Comorbid medical conditions: AOR 1.3, 95% CI 0.9-1.8, p = 0.10.
The income result is worth reading carefully. Low income had a crude OR of 2.1, so it was not irrelevant descriptively. But once the model included age, sex, residence, education, employment, income, psychiatric family history, substance history, comorbidity, and stressful life events, the independent income estimate disappeared.
That pattern can happen when income is entangled with geography, work status, education, household composition, and access to care. It does not prove income is harmless; it shows that this sample did not isolate an independent income effect after adjustment.
Quality of Life Was Lower Across Every Domain
Total WHOQOL-8 score averaged 25.9 with SD 3.9. The lowest mean domain score was environmental circumstances at 5.9, followed by physical well-being at 6.1, subjective well-being at 6.7, and psychosocial well-being at 7.2.1
The depression-quality-of-life link was broad rather than confined to one domain. Total GDS score correlated with total quality of life at r = −0.48, p < 0.001.
Domain correlations were also negative:
- Physical well-being: r = −0.49, p < 0.001.
- Subjective well-being: r = −0.38, p < 0.001.
- Psychosocial well-being: r = −0.38, p < 0.001.
- Environmental circumstances: r = −0.23, p < 0.001.
Negative correlations mean higher depression scores were tied to lower quality-of-life scores. The strongest link was physical well-being, which fits late-life depression: mood, mobility, pain, sleep, appetite, and chronic disease often move together.
Nepal Data Fit a Wider Late-Life Depression Pattern
The result is not isolated. A prior Kavre district community survey in Nepal also found a substantial geriatric depression burden, and a separate Nepal quality-of-life analysis linked aging, rural residence, and health-related factors with lower quality of life.2,3
Internationally, geriatric depression prevalence varies widely because studies differ in age thresholds, instruments, cutoffs, urban-rural mix, medical comorbidity, and whether they screen community samples or clinics. That variability is why this Sudurpaschim estimate should not be treated as “Nepal's one true rate.”
The more durable lesson is operational: late-life depression screening should be embedded where older adults already touch the system, not treated as a specialty-clinic problem.
- Primary care: chronic-disease visits can pair GDS-15 screening with medication review, pain assessment, sleep assessment, and referral when suicide risk or severe impairment is present.
- Community outreach: hill-region screening needs mobile or community-based follow-up because distance, terrain, transportation, family migration, and limited specialty coverage can turn a treatable depressive syndrome into long-running disability.
- Social-support programs: screening is more useful when positive results connect older adults to practical help alongside a diagnostic label.
That is also why quality-of-life measurement belongs beside depression screening. Two older adults can have the same GDS-15 score but very different needs if one is physically limited, isolated, financially dependent, or unable to reach care. The WHOQOL-8 result reminds the reader that the depression number is a doorway into broader geriatric assessment, not the whole assessment.
Limitations of This Nepal Depression Survey
- Cross-sectional design: the survey cannot prove whether depression lowered quality of life, lower quality of life increased depression, or both reinforced each other.
- Screening, not diagnosis: GDS-15 is useful, but it is not a structured diagnostic interview.
- One province: Sudurpaschim Province is important, but it cannot represent every ecological, ethnic, linguistic, and service-access context in Nepal.
- Residual confounding: chronic pain, cognitive status below exclusion threshold, sleep disorders, widowhood, medication burden, and social isolation may not be fully captured.
- Quality-of-life direction: WHOQOL-8 gives a compact snapshot, not a detailed map of finances, care access, family role, disability, or loneliness.
Questions About Geriatric Depression in Nepal
Does 43.9% mean nearly half of older adults in Nepal have major depression?
No. It means 43.9% screened positive on GDS-15 in this province-level sample. A diagnostic interview would likely produce a different estimate.
Should age 75+ adults be prioritized for screening?
Yes. Age ≥75 remained significant after adjustment, and screening is low-burden when paired with primary care or community outreach.
Does the study prove hill residence causes depression?
No. Hill-region residence remained associated with depression, but the mechanism could involve access, geography, social networks, economic conditions, health care, or unmeasured factors.
What should happen after a positive screen?
A positive GDS-15 screen should trigger a practical second step beyond a label. Clinics need to check suicide risk, grief, pain, sleep, medicines, alcohol use, cognition, hearing, mobility, family support, and whether the person can realistically reach follow-up care. In hill-region settings, the access plan may matter as much as the depression score.
How should Nepal clinics use the 43.9% depression finding?
Older-adult depression screening in Nepal should be paired with quality-of-life assessment. The depression score is only part of the burden; physical function, environment, social support, and access to care shape what help is realistic.
What should readers avoid overreading?
The study does not rank every Nepal region or prove that one ecological zone is intrinsically high risk. It identifies a high-burden province sample where age, geography, and quality-of-life impairment point to practical screening needs.
References
- Depression and quality of life among older adults in Far-Western Nepal. Kunwar D, et al. BMC Geriatrics. 2026. doi:10.1186/s12877-026-07478-8
- Prevalence of geriatric depression in the Kavre district, Nepal. Manandhar K, et al. BMC Psychiatry. 2019;19:271. doi:10.1186/s12888-019-2258-5
- Quality of life and its predictors among aging people in urban and rural Nepal. Risal A, et al. Quality of Life Research. 2020;29:3201-3212. doi:10.1007/s11136-020-02593-4
- Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Sheikh JI, Yesavage JA. Clinical Gerontologist. 1986;5:165-173. doi:10.1300/J018v05n01_09
- The World Health Organization Quality of Life assessment position paper. WHOQOL Group. Social Science & Medicine. 1995;41:1403-1409. doi:10.1016/0277-9536(95)00112-K