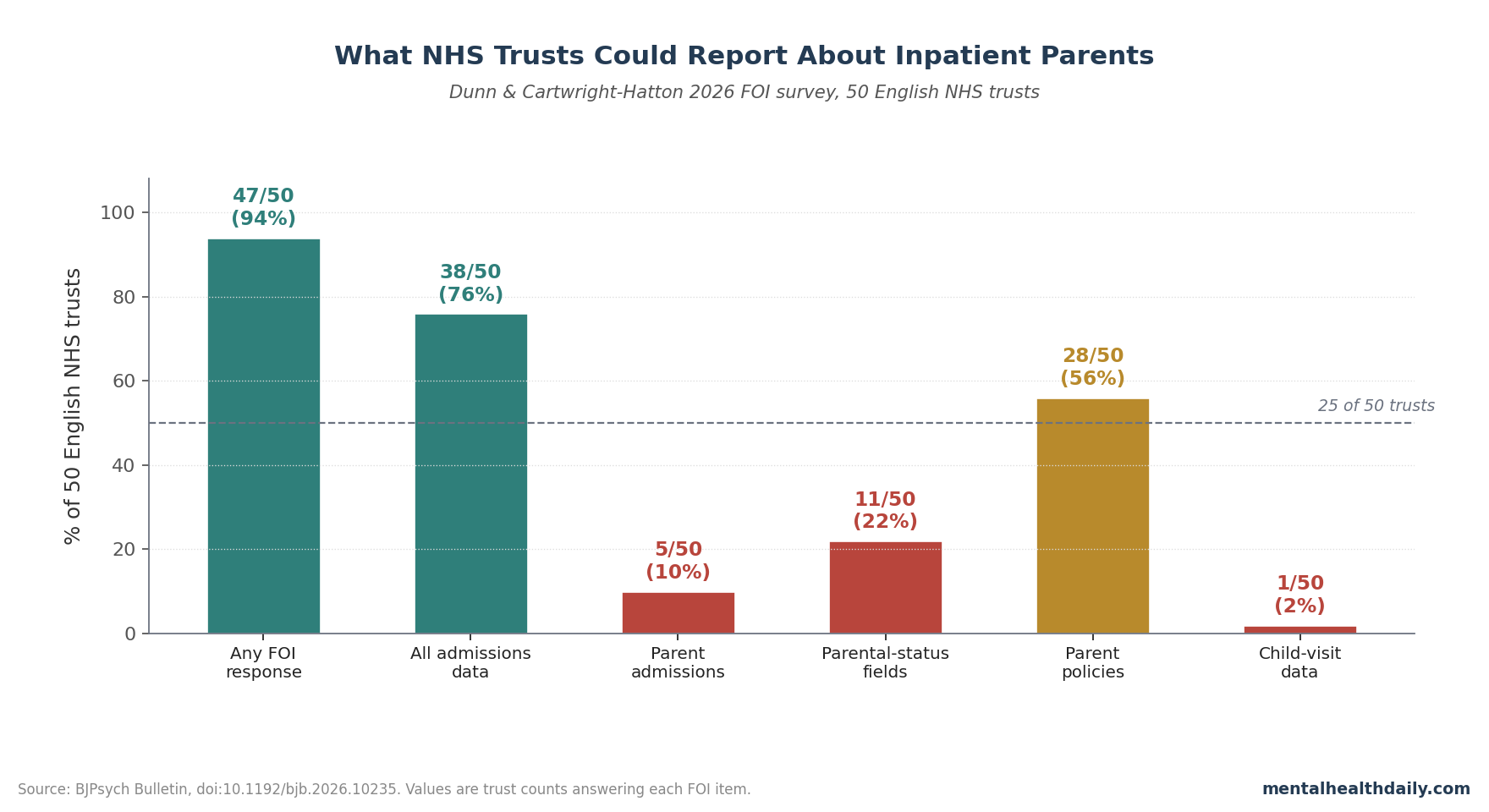
A 2026 Freedom of Information survey of all 50 English NHS trusts providing inpatient psychiatric care found a basic visibility failure: only 5 trusts could say how many psychiatric inpatients were parents, only 11 could describe routine parental-status data collection, and only 1 held child-visit data.1
Research Highlights
- Parent counts were mostly unavailable: 5 of 50 trusts reported parent-admission prevalence, with those limited estimates ranging from 4.3% to 21.0% and averaging 13.9% of inpatients.1
- Parental-status data were not routine: 11 of 50 trusts could describe what information they collected about patients’ children, and no trust captured all 14 listed parental-status items.1
- Policy coverage was incomplete: 28 of 50 trusts returned policies or procedures about inpatient parents, while 18 provided any materials for parents, carers, or children.1
- Child visits were almost invisible: 1 of 50 trusts held child-visit data; it reported 206 high-secure, 142 medium-secure, and 13 low-secure child visits over 2 years, but no visit rate could be calculated.1
- The denominator matters: earlier prevalence work placed parenthood among psychiatric inpatients at 12.3% to 38.5% internationally, and a 2024 Czech inpatient analysis reported 34.6%.3,4
The sharper read is not that every ward refuses family contact. Dunn and Cartwright-Hatton found something more operationally damning: most trusts could not retrieve the minimum data needed to know whether inpatient parents were being identified, whether their children were visiting, or whether parent-support policies existed outside individual case notes.1
Family-focused psychiatric care means adult mental health services recognize that a patient may also be a parent, ask about children and caregiving arrangements, support safe contact during admission, and plan discharge around the family system instead of treating parenting as a side issue. The 2026 FOI survey suggests that this basic infrastructure is still uneven across English inpatient psychiatry.
Only 5 of 50 Trusts Could Report How Many Inpatients Were Parents
Dunn and Cartwright-Hatton sent FOI requests to every English NHS trust providing inpatient psychiatric care, asking for data from 1 January 2018 through 31 December 2019. The pre-COVID-19 window matters because pandemic restrictions would have distorted admission patterns, ward visiting, and family contact.
Of the 50 trusts, 47 provided at least partial information and 3 did not respond at all. Basic all-admission data were easier to retrieve: 38 trusts returned some form of admission count, although not always by ward as requested.1
The parent denominator collapsed. Only 5 trusts could provide meaningful data on how many admitted patients were parents of children under 18.
Among those 5 trusts, identified parenthood ranged from 4.3% to 21.0% of inpatients, with a mean of 13.9%. That mean should not be read as the national NHS prevalence.
It is a thin estimate from the 10% of trusts that could answer.
The paper’s own discussion makes the comparison uncomfortable. The researchers noted that prior international inpatient estimates ranged from 12.3% to 38.5%, and a newer Czech inpatient evaluation found 34.6% parenthood prevalence among hospitalized adults with severe mental illness.3,4
The low 13.9% mean from the 5 English trusts may reflect real differences, under-recording, or both. The FOI design cannot separate those possibilities because the missing data are the finding.
Parental-Status Questions Were Often Safeguarding-Triggered, Not Routine
Parental-status data are the basic admission details that tell a ward whether a patient has children, whether the patient has parental responsibility, where the children are living, which professionals are involved, and whether the parent needs support to maintain contact or explain hospitalization to the child. These questions are not exotic service-development metrics.
They are the minimum dataset for knowing whether a psychiatric inpatient has dependent children affected by admission.
Only 11 trusts could say what parental-status information they routinely collected. Across those trusts, the reported fields included children’s names, ages or dates of birth, legal responsibility, current care arrangements, other agencies involved with the children, other adults in the household, whether children lived with the patient, school or health-visitor details, consent to notify relevant professionals, pregnancy status, parenting-support needs, and risk to children.1
No trust captured all of the listed items. More importantly, some trusts used a safeguarding-triggered model, where detailed questions appeared only after staff had already identified a safeguarding concern.
That flips the logic. A service cannot reliably recognize child welfare needs, child-contact needs, or ordinary parenting-support needs if it first has to identify risk before asking whether the patient has children.
This is where the Mental Health Act Code of Practice point becomes practical rather than decorative. Dunn and Cartwright-Hatton emphasized that inpatient services are expected to support family roles, visits, child-visit policies, and child-understandable information.
If parental-status fields live in case notes, optional forms, or safeguarding branches rather than a centrally retrievable admission dataset, the trust cannot audit whether those expectations are being met.1
28 Trusts Had Policies, But Parent-Facing Materials Were Sparse
Policy evidence was better than prevalence evidence, but still weak for a national service. Dunn and Cartwright-Hatton reported that 28 of 50 trusts returned policies or procedures relating to inpatients who are parents.
That means 22 trusts either had no retrievable policy, did not provide one, or could not identify one through the FOI process.1
The materials trail was thinner. The researchers reported several distinct document types:
- Ward welcome packs: 11 trusts sent inpatient welcome packs, and 8 of those included some reference to parents’ needs.
- Carer materials: 13 trusts sent information sheets for carers of inpatients, but only 8 included reference to inpatient parents or their children.
- Children’s-carer materials: 3 trusts provided information sheets for the carers of inpatients’ children.
- Child-facing resources: 3 trusts provided resources written for children of inpatients.
The reported parent and child content was usually basic. Where policies mentioned child visits, the paper says they generally focused on documentation and risk assessment rather than active facilitation.
In plain terms: the existence of a policy did not prove that children were being helped to visit safely, understand the admission, or maintain a relationship with the hospitalized parent.
Child Visits Were Expected, Yet Almost Never Measured
The child-visit result shows the difference between allowing something and supporting it. Only 1 trust could provide child-visit data, and even that trust could provide data only for secure services.
Over the 2-year period, it reported 206 child visits to high-secure services, 142 to medium-secure services, and 13 to low-secure services.1
Those numbers are real counts, but they are not interpretable as rates. The researchers could not determine how many admissions occurred on those wards, so they could not calculate visits per inpatient, visits per parent, or the share of parents receiving at least 1 child visit.
No trust could answer how many parents received at least 1 visit from a child.
That distinction is operationally huge. A ward may technically permit child visits but have no child-friendly room, no age-appropriate information, no proactive planning, and no way to know whether visits are happening.
Data absence does not prove that every child was blocked from visiting. It does show that child contact was not being managed as a measurable part of inpatient care.
Hospitalized Parents Are Common Enough to Require Routine Systems
The FOI paper should not be read as a niche complaint about a small subgroup. Maybery and Reupert’s review identified parenthood as a routine feature of adult psychiatric services, with inpatient prevalence estimates in the 12.3% to 38.5% range.3
Havelkova et al. later reported 34.6% parenthood prevalence among hospitalized adult patients with severe mental illness in the Czech Republic.4
Dunn et al.’s earlier systematic review of psychiatric inpatients who are parents found a limited intervention literature and recurring reports that inpatient settings often failed to address parenting roles, child contact, and the emotional strain of separation.2 That review makes the FOI findings less surprising.
If parenthood is not reliably identified, tailored interventions will naturally remain patchy.
The child-outcome literature moves the issue beyond adult-service documentation. Bell et al. linked parental psychiatric hospitalization with poor school readiness in children, using population-level data rather than ward anecdote.5
Reupert et al.’s qualitative systematic review also found that family members experience parental hospitalization as confusing, disruptive, and emotionally loaded, especially when children receive little explanation or support.6
The practical inference is not that inpatient teams can eliminate intergenerational psychiatric risk by improving visiting policies. The narrower and more defensible inference is that a service cannot reduce avoidable separation harm if it does not routinely know which patients are parents, where the children are, what contact is safe, and what information children and carers need.
Family-Focused Inpatient Care Starts With Countable Workflows
The 2026 survey points to a basic implementation sequence. It is not glamorous, but it is the difference between policy language and actual service design:
- Ask every adult inpatient about dependent children: parental status should be part of ordinary admission workflow, not a question reserved for visible safeguarding crises.
- Record the same core fields across wards: child age, caregiving arrangement, parental responsibility, child-contact plan, professionals involved, and immediate support needs should be retrievable as structured data.
- Make child-contact planning auditable: trusts should know whether a parent received a child visit, whether a visit was considered and declined, and whether remote contact was arranged when in-person contact was unsuitable.
- Give families usable materials: parent handouts, carer handouts, and child-facing explanations should exist before a crisis admission, not be improvised by each ward.
- Separate risk assessment from family support: child safeguarding is essential, but parenting support is broader than risk management. Many families need explanation, continuity, and planning even when no abuse or neglect concern is present.
Dunn and Cartwright-Hatton suggested that template policies and leaflets would be a relatively easy fix because many trusts were not starting from mature local materials.1 The harder fix is making parental identity visible in the same administrative systems that already track admissions, bed use, and discharge planning.
FOI Data Show System Visibility, Not Family Experience
Freedom of Information surveys test what a public body can retrieve and disclose. They do not directly observe ward practice, interview families, or rate the quality of a child visit.
That limitation matters here because a trust may support a family well in individual cases while still failing to hold centralized data.
The reverse is also true. A trust may possess a policy document without delivering good family support on the ward.
Dunn and Cartwright-Hatton explicitly cautioned that documented policy does not equal lived patient experience. The survey was designed as a broad overview, and the researchers said more detailed quality work on policies, resources, and facilities would be reported separately.1
Several limits keep the article’s conclusion calibrated:
- Time window: the FOI request covered 2018-2019, so later local improvements are possible.
- Jurisdiction: the study focused on England, not Scotland, Wales, or Northern Ireland, which have different health-system structures.
- Incomplete denominator: parent-prevalence estimates came from only 5 trusts, so the 13.9% mean is not a national rate.
- Retrievability problem: failure to answer does not prove no support existed, but it does mean the support was not readily auditable.
Even with those limits, the central result survives. A national service cannot plan parent-sensitive inpatient care if most trusts cannot count inpatient parents, cannot describe routine parental-status fields, and cannot measure child visits.
Questions About NHS Inpatient Parent Support
What exactly did the 2026 FOI survey ask NHS trusts for?
The request asked for total adult psychiatric inpatient admissions, admissions of parents with children under 18, routine parental-status data fields, policies and materials relating to inpatient parents or their children, and child-visit counts for 2018-2019.1
Is the 13.9% parenthood estimate a national NHS rate?
No. It is the mean among the 5 trusts that could report parent-admission data.
Because 45 of 50 trusts could not provide meaningful parent-prevalence data, 13.9% should be treated as a limited retrievable-data estimate, not the national prevalence of inpatient parenthood.1
Does a parent policy mean child visits were actually supported?
Not necessarily. Twenty-eight trusts returned policies or procedures, but the paper reports that child-visit content often centered on documentation and risk assessment.
A policy is useful only if wards have child-appropriate space, staff workflow, family information, and a way to track whether contact happened.1
What did the single child-visit dataset show?
One trust reported secure-service child visits over 2 years: 206 high-secure visits, 142 medium-secure visits, and 13 low-secure visits. The researchers could not calculate a rate because the dataset did not include the necessary admission denominator for those wards.1
How does this differ from mother-and-baby unit care?
Mother-and-baby units address a specific perinatal situation: keeping a mother and infant together during severe postnatal psychiatric illness. Dunn and Cartwright-Hatton studied the broader adult inpatient system, including parents of older children, fathers, stepparents, foster parents, and other adults with formal child-care responsibilities.1
What should a hospitalized parent or relative ask the ward?
Ask whether parental status has been recorded, who is documenting the child-contact plan, whether child visits are possible and where they occur, what information is available for the child or carer, and how discharge planning will handle the return to parenting. The FOI findings show why these questions cannot be assumed to happen automatically.1
References
- Dunn A, Cartwright-Hatton S. Support for parents in in-patient psychiatric care in English NHS trusts: Freedom of Information survey. BJPsych Bulletin. 2026. doi:10.1192/bjb.2026.10235
- Dunn A, Christiansen H, Elsby-Pearson C, Kramer J, Swinburn E, Platt B. Psychiatric in-patients who are parents: what interventions are tailored to their needs and how do they experience care? A systematic review and data synthesis. BJPsych Open. 2023;9:e111. doi:10.1192/bjo.2023.67
- Maybery D, Reupert AE. The number of parents who are patients attending adult psychiatric services. Current Opinion in Psychiatry. 2018;31(4):358–362. doi:10.1097/YCO.0000000000000427
- Havelkova A, Havelka D, Koros Bartosova K. Prevalence of parenthood among hospitalized adult patients with severe mental illness: a quantitative data analysis. Frontiers in Psychiatry. 2024;15:1386842. doi:10.3389/fpsyt.2024.1386842
- Bell MF, Bayliss DM, Glauert R, Harrison A, Ohan JL. Children of parents who have been hospitalised with psychiatric disorders are at risk of poor school readiness. Epidemiology and Psychiatric Sciences. 2019;28(5):508–520. doi:10.1017/S2045796018000148
- Reupert A, Tchernegovski P, Chen L, Huddle M. Experiences of family members when a parent is hospitalized for their mental illness: a qualitative systematic review. BMC Psychiatry. 2023;23:56. doi:10.1186/s12888-023-04530-4