A 337-person SYNGAP1-DEE registry preprint found caregiver-reported autistic behavior scores linked most strongly to atypical absence seizures (n = 77; FDR-adjusted p = .001), while peak seizure-frequency ratings were not detectably associated with those behavior scores.1
Research Highlights
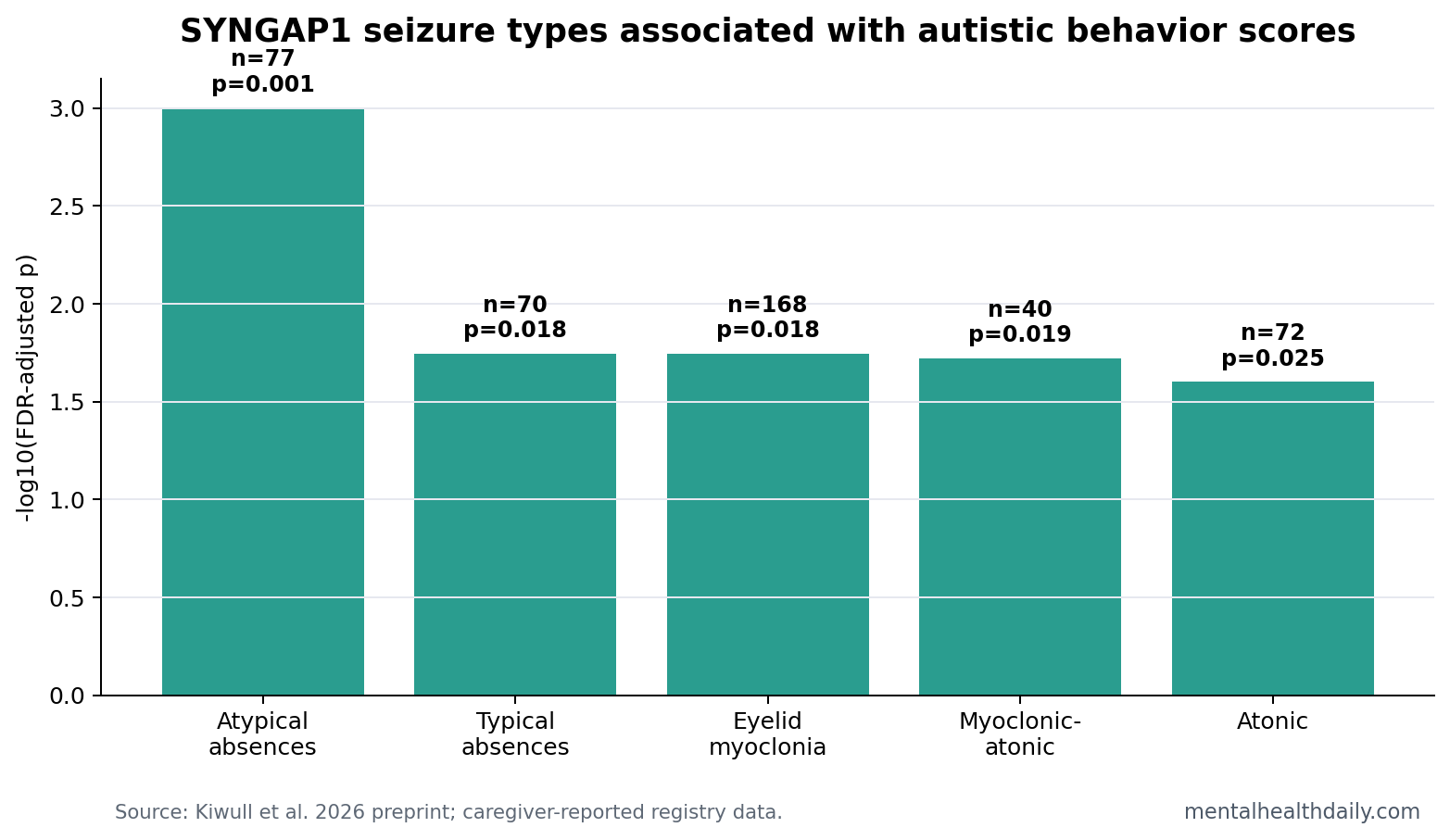
- Seizure type carried the signal: atypical absences were associated with higher caregiver-reported autistic behavior scores in 77 SYNGAP1-DEE participants (FDR-adjusted p = .001).1
- Frequency did not explain the pattern: peak seizure-frequency ratings were not detectably associated with autistic behavior scores, including atypical absences (p = .744).1
- Several generalized patterns also stood out: typical absences (n = 70; p = .018), eyelid myoclonia (n = 168; p = .018), myoclonic-atonic seizures (n = 40; p = .019), and atonic seizures (n = 72; p = .025) were associated after FDR correction.1
- The cohort was large for a rare disorder: researchers analyzed 337 participants with complete epilepsy and behavior data from 522 registry participants.1
- Preprint limits are real: the study was cross-sectional, caregiver-reported, and not yet peer reviewed, so it cannot prove that seizure semiology causes autistic behaviors.1
SYNGAP1-related developmental and epileptic encephalopathy (SYNGAP1-DEE) is a rare genetic neurodevelopmental condition caused by pathogenic variants affecting SYNGAP1, a gene involved in synaptic signaling and brain development. Children and adults with SYNGAP1-DEE often have developmental delay, intellectual disability, epilepsy, sleep problems, and autism-related behaviors.2
Seizure semiology means the observable form of a seizure: what the body, awareness, eyelids, posture, or behavior does during the event. The 2026 preprint asks whether the type of seizure carries more behavioral information than how often caregivers report seizures occurring.
Atypical Absences Were the Strongest Autistic-Behavior Signal
Kiwull et al. used the PATRE registry for SYNGAP1 and restricted analysis to 337 participants with complete epilepsy and behavior questionnaire data.1 Epilepsy was reported in 259 of them. Caregiver-reported autistic behaviors were measured on a 1 to 5 scale, and seizure frequency was captured with a 9-point ordinal caregiver rating.
Atypical absence seizures are generalized seizures involving impaired awareness, often with a less abrupt beginning or ending than typical absences. In this analysis, atypical absences showed the most robust association with higher autistic behavior scores after false-discovery-rate correction.
False-discovery-rate correction is a statistical adjustment used when researchers test many related comparisons. It lowers the chance that a result survives only because the study ran many tests. The atypical-absence association survived that correction at p = .001.
- Atypical absences: n = 77; FDR-adjusted p = .001.
- Typical absences: n = 70; FDR-adjusted p = .018.
- Eyelid myoclonia: n = 168; FDR-adjusted p = .018.
- Myoclonic-atonic seizures: n = 40; FDR-adjusted p = .019.
- Atonic seizures: n = 72; FDR-adjusted p = .025.
Peak Frequency Ratings Were Not the Behavioral Readout
The frequency result is the useful correction. It would be easy to assume that more seizures should map to more autistic behaviors, but the analysis did not find a detectable correlation between peak seizure-frequency ratings and caregiver-reported autistic behavior scores across the semiologies.
For atypical absences, the frequency association was p = .744. For eyelid myoclonia, it was p = .096. Those values do not prove frequency is irrelevant in every clinical sense. They show that this ordinal caregiver-reported peak-frequency metric did not carry the same behavioral information as seizure type.
Clinical translation: asking “how often are seizures happening?” may miss a behavior-relevant phenotype if the seizure type reflects different thalamocortical network involvement. A child with a lower-frequency semiology tied to awareness interruption may look behaviorally different from a child with frequent events of another type.
The frequency finding should be read narrowly. The analysis used a caregiver-rated peak-frequency scale, separate from continuous electroencephalography, seizure-duration totals, medication-adjusted burden, or time-varying counts.
A child with frequent seizures may still have sleep disruption, injury risk, missed learning time, and family stress. The narrower result is that peak frequency ratings did not explain autistic behavior scores the way seizure type did in this registry dataset.1
For clinicians, the practical move is better history-taking: document seizure type, awareness change, timing, sleep context, and medication changes alongside frequency. A count alone can flatten biologically different events into the same severity bucket and hide patterns families can describe clearly.
Thalamocortical Seizures Fit the Network-Level Interpretation
The researchers interpreted atypical absences as a marker of generalized thalamocortical network dysfunction. Thalamocortical networks are loops connecting the thalamus, a deep relay hub, with the cerebral cortex. These loops help regulate awareness, sensory processing, attention, and rhythmic brain activity.
That network framing is more useful than treating autism-related behaviors as a generic consequence of epilepsy. SYNGAP1 affects synaptic signaling, so a seizure pattern that reflects particular network instability may index broader developmental circuitry differences.
Earlier SYNGAP1 literature already linked pathogenic variants with epilepsy, intellectual disability, developmental delay, and autism-related traits.2,3 The 2026 registry analysis adds a more specific claim: in this dataset, the behavioral association concentrated around semiology rather than peak frequency.
Replication target: if atypical absences and related generalized events repeatedly track behavior across cohorts, semiology could become part of a phenotype stratification system.
If the signal disappears after adjustment for developmental level, sleep, medication, or electroencephalography burden, then the registry association would be better treated as a marker of broader severity rather than a distinct behavioral pathway.
Either result would improve counseling because it would replace vague severity language with a measurable epilepsy-behavior model. Families need that specificity when symptoms change over time.
Caregiver-Reported Registry Data Need Guardrails
Evidence-strength note: this was a retrospective cross-sectional registry analysis and a medRxiv preprint. It can identify associations inside caregiver-reported data, but it cannot establish causality, guide medication changes, or show that suppressing atypical absences will reduce autistic behaviors.
Caregiver report is still valuable in rare disorders. Families observe seizures, sleep, attention, communication, and behavior across settings that clinic visits miss. The limitation is measurement precision: caregiver frequency ratings may not capture electroencephalography burden, seizure duration, medication effects, developmental level, or clustering.
The right read is calibrated. Semiology deserves attention as a phenotype marker. Frequency should not be discarded, but it should not be treated as the only epilepsy variable worth measuring in SYNGAP1-DEE.
Better Phenotyping Would Separate Count, Type, and Context
Future SYNGAP1 studies should avoid collapsing epilepsy into a single severity variable. A useful prospective design would record seizure semiology, event duration, clustering, medication exposure, sleep disruption, electroencephalography patterns, developmental level, and caregiver-rated behavior at repeated time points.
Count: frequency still has clinical value because frequent seizures can disrupt sleep, school, attention, safety, and family routines. The 2026 analysis only says peak caregiver-rated frequency did not explain autistic behavior scores in this dataset.
Type: semiology may point toward specific network involvement. Absence-like and atonic events may index different thalamocortical or motor-network vulnerability than focal or tonic-clonic events.
Context: behavior scores can change with sleep, medication adverse effects, developmental stage, communication demands, and caregiver stress. Without those covariates, a seizure-behavior association can be real but still incomplete.
The practical payoff is more precise natural-history research. Families often ask whether epilepsy features explain behavior, and clinicians need better answers than “seizures are common in SYNGAP1.” This preprint suggests the next answer should name the seizure type, the measurement method, and the limits of caregiver-reported frequency.
One useful design would pair caregiver diaries with ambulatory EEG and repeated behavior ratings. Diaries would preserve family-observed context, EEG would reduce misclassification of seizure burden, and repeated ratings would show whether behavior shifts after changes in sleep, medication, seizure pattern, or developmental demands.
Another useful design would compare SYNGAP1 with other developmental and epileptic encephalopathies. If atypical absences predict behavior across several genetic epilepsies, the result may reflect a broader thalamocortical pathway. If the association is SYNGAP1-specific, the gene’s synaptic biology becomes more central to interpretation.
Families should not be asked to translate this into treatment decisions alone. The safer near-term use is documentation: name the seizure type, record the context, track behavior with the same scale over time, and bring the pattern to neurology and developmental-care visits.
The result may also change how clinicians phrase uncertainty. Saying “behavior is part of SYNGAP1” is accurate but not very useful. Saying “some seizure types may index the same thalamocortical systems involved in behavior” gives families a testable framework without promising that seizure control will normalize autism-related traits.
That distinction protects both sides of care. It prevents therapeutic nihilism, where behavior is treated as untouchable background, and it prevents overpromising, where every seizure medication adjustment is expected to produce broad social-communication change.
It also gives rare-disease registries a concrete target for cleaner next-wave data collection.
Questions About SYNGAP1 Seizure Semiology and Autistic Behaviors
Does this mean atypical absences cause autism in SYNGAP1-DEE?
No. The study found an association between atypical absences and caregiver-reported autistic behaviors. Shared neurodevelopmental circuitry, reporting patterns, or disease severity could contribute.
Why is seizure frequency not enough?
A frequency count treats seizures as interchangeable. Semiology captures what kind of network event is happening, which may be more informative for behavior in some genetic epilepsies.
Should treatment change based on this preprint?
No. The paper has not been peer reviewed and does not test treatment. It supports better phenotyping and prospective studies, not clinical changes by itself.
References
- Kiwull L, et al. Beyond Seizure Burden: Seizure Semiology, but not Frequency, is Associated with Caregiver-Reported Autistic Behaviors in SYNGAP1-DEE. medRxiv. 2026. doi:10.64898/2026.04.19.26351217
- Berryer MH, et al. Mutations in SYNGAP1 cause intellectual disability, autism, and a specific form of epilepsy by inducing haploinsufficiency. Human Mutation. 2013. https://doi.org/10.1002/humu.22331
- Vlaskamp DRM, et al. SYNGAP1 encephalopathy: A distinctive generalized developmental and epileptic encephalopathy. Neurology. 2019. https://doi.org/10.1212/wnl.0000000000007895
- Jimenez-Gomez A, et al. Phenotypic characterization of individuals with SYNGAP1 pathogenic variants reveals a potential correlation between posterior dominant rhythm and developmental progression. Journal of Neurodevelopmental Disorders. 2019. https://doi.org/10.1186/s11689-019-9276-y