A pilot randomized trial involving 71 refugees with posttraumatic stress disorder found large symptom improvement after narrative exposure therapy-based care, but adding refugee-adapted emotion-regulation training before narrative exposure therapy did not outperform supportive problem-solving before narrative exposure therapy in the full sample.1
Research Highlights
- 71 refugees were randomized: 35 received STAIR-R plus narrative exposure therapy, and 36 received supportive problem-solving plus narrative exposure therapy.1
- PTSD symptoms dropped in both arms: clinician-rated PTSD severity fell from pretreatment to posttreatment by 15.50 CAPS-5 points across treatment arms, with p < .001.1
- No overall add-on advantage appeared: STAIR-R did not produce significant between-arm superiority over supportive problem-solving at midtreatment, posttreatment, or 3-month follow-up.1
- A high-insecurity subgroup favored STAIR-R: refugees with temporary visas or complete family separation had larger self-reported PTSD, depression, emotion-regulation, relationship, and environmental quality-of-life advantages with STAIR-R than with supportive problem-solving.1
- Evidence remains preliminary: this was a 71-person pilot randomized trial, and the high-insecurity subgroup included 16 people, so the subgroup result needs an adequately powered trial designed around post-migration insecurity.
Narrative exposure therapy is a trauma-focused psychotherapy that asks a person to build a chronological life narrative, including traumatic events, so fragmented trauma memories can be placed into autobiographical context. STAIR-R, or Skills Training in Affective and Interpersonal Regulation for Refugees, teaches emotion regulation and relationship skills before trauma narration so refugees can tolerate trauma-focused work while facing displacement stress.
71 Refugees Received 13 Sessions of Phase-Based PTSD Care
Nickerson et al. enrolled adult Arabic-speaking refugees and asylum seekers in Australia who met criteria for posttraumatic stress disorder. Mean age was 46.79 years, 66.2% were female, 93.0% spoke Arabic as their main language, and 69.0% met criteria for current major depressive disorder.1
- STAIR-R plus NET: 6 sessions of refugee-adapted emotion-regulation and interpersonal skills, followed by 7 sessions of narrative exposure therapy.
- SPS plus NET: 6 sessions of supportive problem-solving, followed by the same 7-session narrative exposure therapy sequence.
- Delivery context: 97.2% of participants worked with an interpreter, and 80.3% received online or hybrid therapy during pandemic-era restrictions.
- Completion: 54 of 71 participants, or 76.1%, completed all 13 therapy sessions.
Supportive problem-solving is an active comparator, not a waitlist. It gives time, therapist contact, practical support, and structured attention before trauma processing. That comparator makes the trial more informative because any STAIR-R advantage had to exceed another credible preparatory treatment.
Both Therapy Sequences Produced Large PTSD Improvements
Clinician-rated PTSD symptoms were measured with the Clinician-Administered PTSD Scale for DSM-5, a structured interview that produces a severity score for PTSD symptoms. Across the full sample, CAPS-5 scores fell substantially from pretreatment to posttreatment, with a time coefficient of B = −15.50, standard error 2.13, and p < .001.1
Follow-up durability: pretreatment to 3-month follow-up change remained large, with B = −14.50, standard error 2.13, and p < .001. Within-arm Hedges g values for CAPS-5 change were −1.61 at posttreatment and −1.41 at follow-up for STAIR-R plus NET, compared with −1.64 at posttreatment and −1.54 at follow-up for supportive problem-solving plus NET.1
Self-reported PTSD symptoms also improved. PCL-5 scores decreased at midtreatment, posttreatment, and follow-up, including a posttreatment coefficient of B = −11.25 with p < .001.1
Overall interpretation: the trial supports narrative exposure therapy-based care for refugees with PTSD, including interpreter-mediated and hybrid delivery. It does not show that STAIR-R should replace supportive problem-solving as the default preparatory phase for all refugee patients.
High Post-Migration Insecurity May Be the STAIR-R Signal
Subgroup definition: a prespecified high-insecurity subgroup included 16 refugees who had temporary visa status or were separated from all family members. In that subgroup, STAIR-R plus NET produced larger gains than supportive problem-solving plus NET on several self-reported outcomes.1
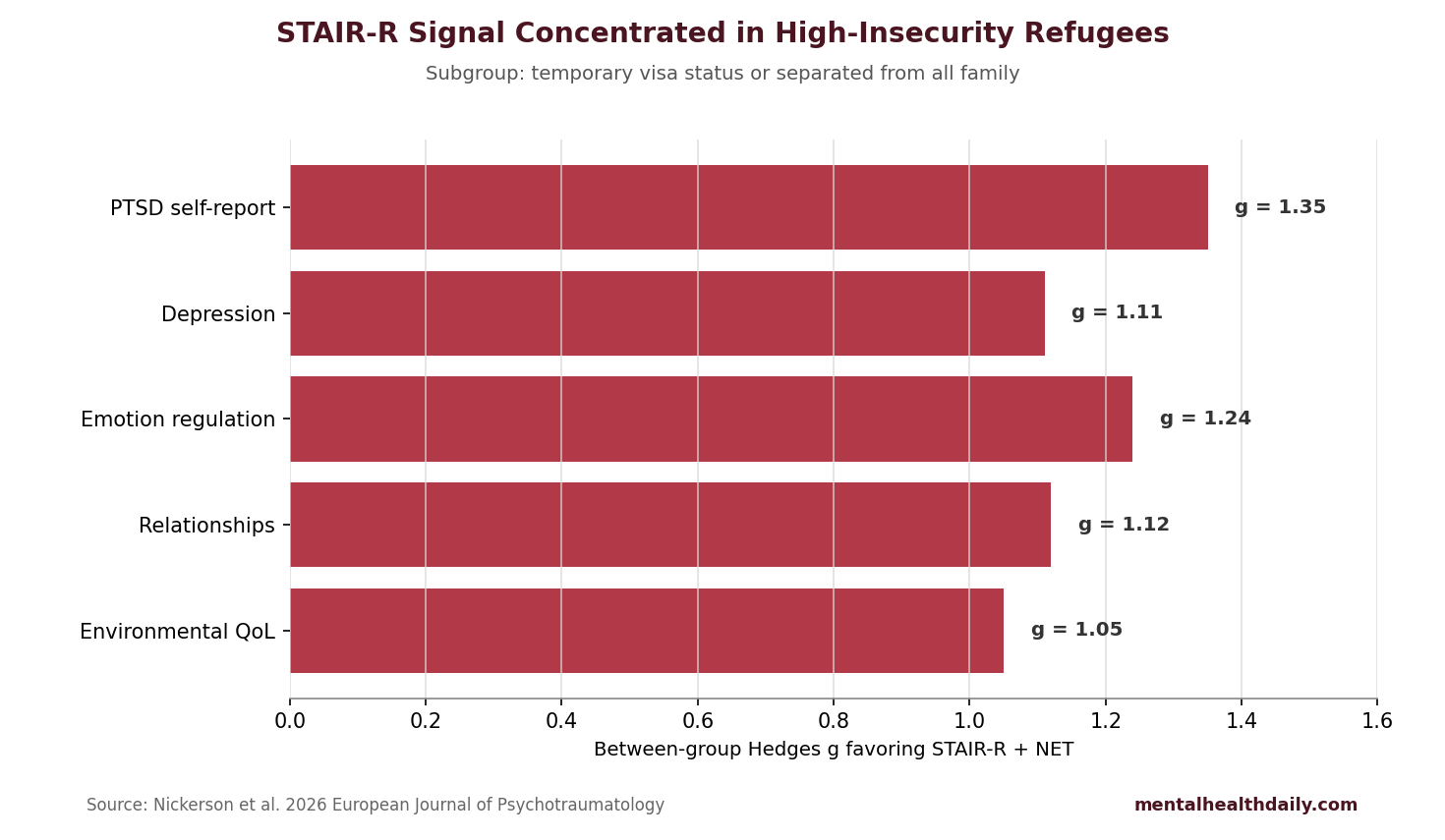
The largest subgroup advantages were self-reported PTSD symptoms, emotion-regulation difficulties, depression, relationship difficulties, and environmental quality of life. The PTSD self-report advantage was g = 1.35, depression was g = 1.11, emotion-regulation difficulties were g = 1.24, relationship difficulties were g = 1.12, and environmental quality of life was g = −1.05 because lower scoring direction on that scale represented worse environmental quality of life.1
Why insecurity may change treatment response: refugees facing family separation, uncertain visas, unsafe housing, or legal precarity may need practical emotion-regulation and interpersonal tools before trauma narration. Skills practice may reduce arousal, avoidance, and conflict enough for trauma-focused sessions to work with less destabilization.
Adjacent Evidence Supports Trauma-Focused Care but Leaves Sequencing Open
Broader evidence: meta-analytic evidence has supported narrative exposure therapy for posttraumatic stress disorder in refugees and asylum seekers, including trials in unstable post-conflict and resettlement settings.2 Broader reviews of psychosocial interventions have also found benefits for PTSD symptoms in refugees, although study quality, cultural adaptation, interpreter use, and follow-up length vary widely.3
Sequencing remains unsettled: phase-based trauma care makes clinical sense when emotion dysregulation, dissociation, housing insecurity, or current threat interferes with trauma processing. Direct evidence that skills-first care beats credible supportive preparation for all refugees is thinner than the clinical intuition suggests.
Nickerson et al. previously reported that emotion dysregulation helped connect trauma exposure and post-migration living difficulties to psychological symptoms in refugees.4 That background makes the high-insecurity subgroup signal biologically and clinically plausible, but plausibility cannot substitute for a trial powered to test the subgroup.
Evidence-Strength Note for This Pilot Trial
What the design supports: this randomized design can compare 2 active therapy sequences under pilot-trial conditions. It can show feasibility, symptom trajectories, dropout, adverse events, and preliminary subgroup patterns.
Design limits: the sample was small, the high-insecurity subgroup included only 16 participants, and subgroup effect sizes are unstable when a few people can move the estimate. The trial cannot determine whether STAIR-R is superior for all refugees with PTSD or whether post-migration insecurity should become a formal treatment-selection rule.
No adverse events or serious adverse events were recorded, which supports feasibility. Safety in this sample does not remove the need for careful clinical monitoring when trauma-focused therapy is delivered to refugees who face ongoing threat, legal uncertainty, suicidality, psychosis, severe substance use, or domestic violence.
How Clinicians Can Use This Without Overselling STAIR-R
For many refugees with PTSD, the clearest evidence-based anchor remains trauma-focused psychotherapy delivered in a way the person can actually access: language support, flexible scheduling, cultural humility, and attention to current living stressors. Narrative exposure therapy has a stronger evidence base than any single preparatory package.
Clinical fit: STAIR-R may deserve priority when current insecurity, family separation, interpersonal conflict, or affective instability threatens engagement with trauma narration. Supportive problem-solving may be enough when a person is ready for trauma processing and mainly needs practical support before beginning narrative exposure.
Implementation note: refugee PTSD care also needs flexible scheduling, interpreter quality, legal-stress awareness, and coordination with housing or asylum support. Those practical conditions can decide whether a therapy sequence is usable before symptom-score differences become visible.
Future trials should report retention, interpreter continuity, online privacy problems, and post-migration stress changes alongside PTSD scores. Those measures would show whether preparatory skills help people stay engaged with trauma-focused work.
- Use skills when arousal blocks therapy: emotion-regulation practice can reduce dropouts driven by panic, anger, shame, or shutdown.
- Use problem-solving when logistics block therapy: housing, appointments, legal paperwork, and family contact can become treatment barriers.
- Keep trauma work central: both trial arms received narrative exposure therapy, and both arms improved substantially.
Interpreter-Mediated and Online Delivery Deserve Attention
Nearly all participants worked through interpreters, and most therapy was delivered online or in a hybrid format. Those details are not side conditions for refugee PTSD care. Language access, internet access, privacy at home, therapist-interpreter coordination, and trust in remote sessions can determine whether an evidence-based therapy reaches the people who need it.
Implementation point: a refugee PTSD service should not treat the psychotherapy protocol as the only active ingredient. The delivery system also matters: trained interpreters, trauma-informed scheduling, stable video access, child-care flexibility, and therapist skill with uncertainty around visas and family separation. A strong protocol can fail if the surrounding system makes attendance or disclosure unsafe.
- Interpreter quality: trauma narration requires accuracy, pacing, and emotional containment beyond literal translation.
- Remote privacy: online therapy can improve reach, but it can also expose people to interruptions or surveillance fears at home.
- Legal insecurity: visa uncertainty can keep threat active while therapy is trying to process past threat.
Questions About STAIR-R and Refugee PTSD
Did STAIR-R beat supportive problem-solving overall?
No. STAIR-R plus narrative exposure therapy did not show significant superiority over supportive problem-solving plus narrative exposure therapy across the full randomized sample.
Who may benefit most from STAIR-R?
The pilot subgroup signal pointed to refugees facing temporary visa status or complete family separation. That pattern needs confirmation in a larger trial.
Does this weaken narrative exposure therapy?
No. Both arms received narrative exposure therapy after preparation, and both arms had large PTSD symptom reductions.
References
- Emotion regulation skills training as an adjunctive treatment to narrative exposure therapy for PTSD in refugees: a pilot randomized controlled trial. Nickerson A, Liddell BJ, Keegan D, et al. European Journal of Psychotraumatology. 2026. doi:10.1080/20008066.2026.2648941
- The effectiveness of narrative exposure therapy: a review, meta-analysis and meta-regression analysis. Lely JCG, Smid GE, Jongedijk RA, Knipscheer JW, Kleber RJ. European Journal of Psychotraumatology. 2019;10:1550344. doi:10.1080/20008198.2018.1550344
- Psychosocial interventions for post-traumatic stress disorder in refugees and asylum seekers resettled in high-income countries: systematic review and meta-analysis. Nosè M, Ballette F, Bighelli I, et al. PLOS ONE. 2017;12:e0171030. doi:10.1371/journal.pone.0171030
- The role of emotion regulation in the relationship between trauma exposure and mental health in refugees. Nickerson A, Bryant RA, Schnyder U, et al. Journal of Affective Disorders. 2015;173:166–172. doi:10.1016/j.jad.2014.10.043