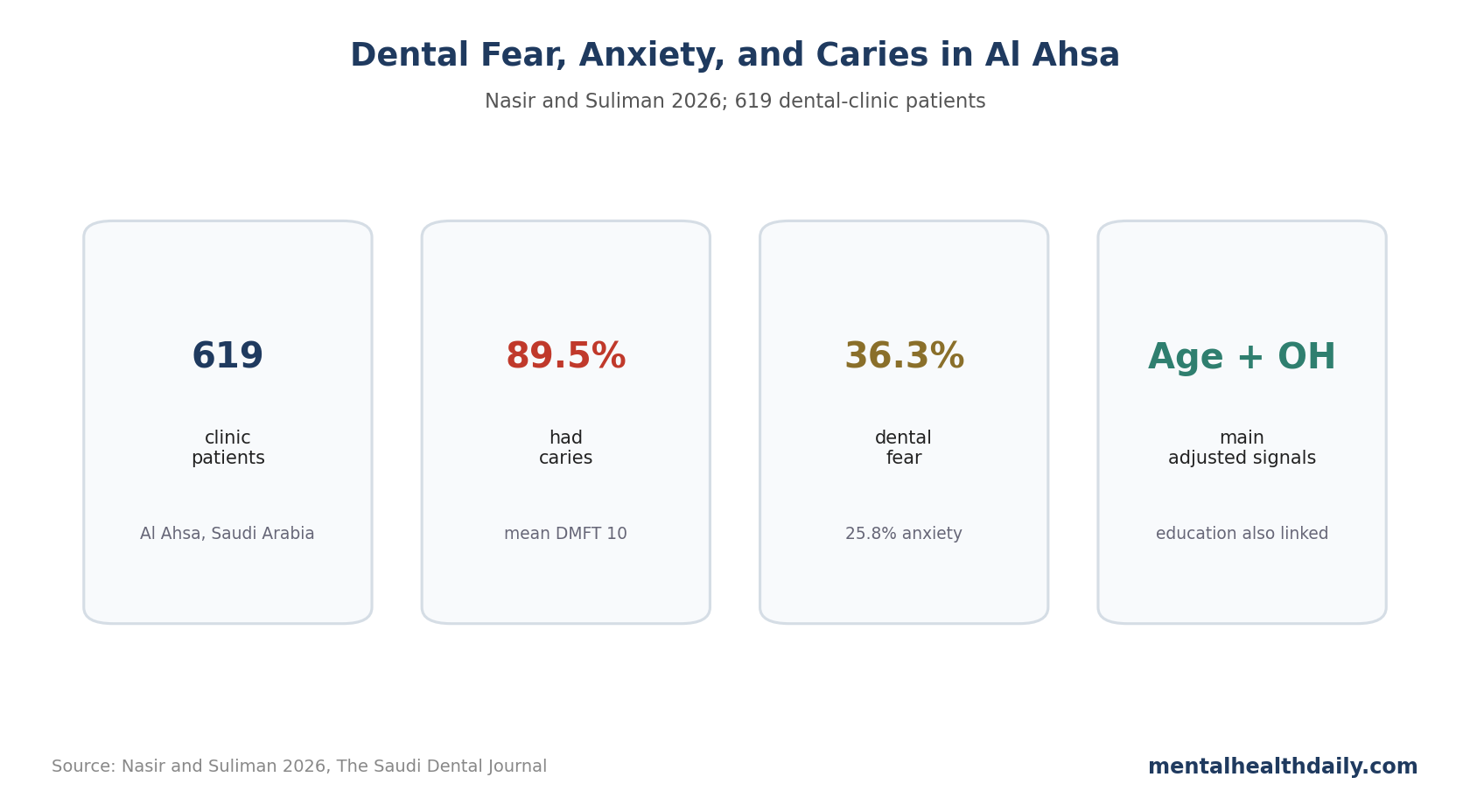
A Saudi dental-clinic study found very high caries burden, but dental fear and anxiety were not the main adjusted explanation for dental caries. In 619 Al Ahsa patients, 89.5% had caries, 36.3% reported dental fear, and 25.8% reported anxiety; age, education, and oral hygiene carried a stronger caries signal than fear or anxiety.1
Research Highlights
- Caries prevalence was high: 89.5% of 619 dental-clinic patients had dental caries, with mean Decayed, Missing, and Filled Teeth (DMFT) score of 10.1
- Fear and anxiety were common: 36.3% reported dental fear and 25.8% reported anxiety, with fear and anxiety strongly correlated with each other.1
- Adjusted caries predictors were more behavioral-demographic: older age, lower education, and poor oral hygiene remained associated with caries in the final model.1
- Dental fear did not explain DMFT: in the linear model, dental fear was not associated with DMFT, and anxiety did not remain a main caries predictor after adjustment.1
- The 619-patient clinic sample limits prevalence claims: hospital-based dental samples can overestimate disease burden because participants are already seeking care.
Dental anxiety can reduce dental attendance, worsen avoidance, and complicate care. This study adds a useful calibration: fear and anxiety were present, but they did not outperform oral hygiene, age, and education as explanations for caries in this clinic cohort.
619 Al Ahsa Dental-Clinic Patients Had High DMFT Scores
Nasir and Suliman conducted a cross-sectional study from September to December 2022 in Al Ahsa, Saudi Arabia. Dental caries were assessed clinically using the Decayed, Missing, and Filled Teeth (DMFT) index, while oral hygiene, dental fear, and anxiety were measured with structured instruments.1
- Sample: 619 patients, mean age 29.46 years, 63.2% male.
- Caries burden: 89.5% had caries; mean DMFT was 10, with standard deviation 7.6.
- Severe caries concentration: significant caries index (SiC30) averaged 18.
- Oral hygiene: 28.1% had poor oral hygiene.
DMFT is a cumulative dental disease measure. It captures active decay plus teeth missing or filled because of prior caries experience.
Fear and Anxiety Were Common but Not the Main Caries Drivers
Fear and anxiety were strongly related to each other, with a correlation of r = 0.70. That makes intuitive sense: a person who fears dental care is more likely to feel anxious about the visit.1
DMFT correlated with age and oral hygiene level, but not meaningfully with fear or anxiety. In the linear regression, age and oral hygiene were significant predictors of DMFT. Fear and anxiety were not.
The binary caries model pointed in the same direction after adjustment: older age, lower education, and poor oral hygiene remained stronger caries indicators than dental fear or anxiety. The abstract reported older age AOR = 3.3, lower education AOR = 0.4 for university/above vs. lower education, and oral hygiene AOR = 0.4 for better hygiene vs. poor hygiene.1
Clinic-Based Sampling Can Inflate Caries Prevalence
The 89.5% caries prevalence is striking, but it should not be read as a population prevalence for all adults in Al Ahsa. Hospital-based dental samples are enriched for people who already need dental care.
Nasir and Suliman explicitly noted this limitation. A population-based sample would include more people without active complaints and would likely produce a lower, more generalizable prevalence estimate.1
Still, the DMFT value is clinically useful inside the sampled setting. It tells dental clinics that many patients arrive with substantial cumulative disease, and that preventive education cannot focus only on anxiety reduction.
Dental Anxiety Still Matters for Attendance and Treatment Experience
The absence of an adjusted caries association does not make dental anxiety irrelevant. Dental fear can still shape avoidance, missed appointments, pain expectations, procedure tolerance, and the need for behaviorally sensitive care.3
The outcome distinction is specific: anxiety may shape attendance behavior and patient experience more than it explains DMFT in a clinic sample where age, education, and hygiene dominate the disease measure.
For dental services, the practical approach is integrated: reduce fear and pain during care, but keep prevention anchored in brushing, fluoride, diet, regular attendance, and early treatment.
Prevention Should Separate Avoidance, Hygiene, and Disease Burden
Dental anxiety can still be part of a prevention strategy even if it was not the dominant adjusted caries predictor. It may operate earlier in the pathway: fear can reduce routine visits, delay treatment, and make people wait until pain forces care.
Once a clinic sample is assembled, the relationship can look weaker or distorted. People with high fear who finally attend may already differ from high-fear people who never come in. People without fear may attend because disease is severe. Clinic-based anxiety-caries correlations can therefore look counterintuitive even when fear still delays care in the broader population.
For prevention, the categories should stay separate:
- Disease burden: DMFT and active lesions measure cumulative dental damage and current treatment needs.
- Hygiene behavior: brushing, fluoride exposure, diet, and early restorative care address caries risk directly.
- Anxiety and access: gentle communication, predictable procedures, topical anesthesia, behavioral support, and staged appointments help fearful patients keep attending care.
- Exposure history: education and age shape years of risk, health literacy, appointment flexibility, and access to prevention.
A clinic can act on all 4 without pretending they are the same.
Anxiety-only explanations are too narrow. The adjusted model argues for a broader prevention package, not for ignoring anxious patients. Dental fear can still block attendance, pain control, and trust even when it is not the strongest statistical explanation for DMFT in this sample.
DMFT Is Cumulative, So Current Anxiety May Be the Wrong Timing
Timing can scramble the anxiety-caries relationship. DMFT reflects years of decay, missing teeth, and restorations. A current anxiety score measures how the person feels now.
Several pathways can lead to the same clinic snapshot:
- Caries before fear: someone may have developed decay before dental fear emerged.
- Fear after treatment: another person may have become fearful after painful treatment for existing disease.
- Hidden avoidance: people with the highest fear may be missing from a clinic sample because they never scheduled care.
A cross-sectional design cannot separate those paths.
DMFT also weights old and current disease together. A filled tooth from years earlier, a tooth missing because of past caries, and a new untreated lesion all count inside the cumulative score, but they can come from different moments in the anxiety-care pathway.
Longitudinal research would be more informative. It could test whether baseline dental fear predicts missed preventive visits, delayed care, new untreated decay, emergency visits, or treatment noncompletion over time.
For now, the clinic-level takeaway is: oral-hygiene intervention and prevention should stay central, and fear-sensitive care should be promoted because it helps anxious patients remain engaged long enough to receive prevention and treatment.
Measurement of Fear and Anxiety May Have Blunted Associations
Nasir and Suliman used a modified dental fear and anxiety questionnaire with fewer response options than some standard instruments. Narrow response scales can reduce variability, which makes it harder to detect graded relationships with disease burden.
Future studies should compare several measurement approaches: a validated dental anxiety scale, dental avoidance history, prior traumatic dental experience, pain expectation, missed appointment records, and longitudinal new-caries outcomes. A richer fear measure may show relationships that a short clinic questionnaire cannot.
Education May Be a Proxy for Several Caries Pathways
Education was associated with caries in the adjusted model, but education itself is rarely the direct biological cause. It can stand in for health literacy, income, access to preventive care, diet, fluoride exposure, appointment flexibility, and familiarity with dental systems.
Access response: make preventive care easier to access, explain risk clearly, reduce appointment fear, and support hygiene routines that people can actually maintain.
Population-Based Follow-Up Would Clarify the Counterintuitive Cross-Tabs
One surprising crude pattern was that people with no anxiety or fear appeared more likely to have caries in some cross-tab results. That should be treated as a sampling and confounding warning, not as evidence that fear protects teeth.
A population-based cohort could measure baseline dental fear, attendance patterns, hygiene, sugar intake, fluoride exposure, socioeconomic status, and new caries over time. That design would show whether anxiety predicts avoidance first and disease later.
Dental clinics can also use fear screening to tailor the visit itself: explain steps before procedures, check pain control early, offer breaks, and avoid shaming language. Those changes may not lower DMFT overnight, but they can keep patients engaged long enough for prevention to work.
Questions About Dental Anxiety and Caries
Did anxiety protect against caries in this study?
No. Some crude cross-tabs looked counterintuitive, but the adjusted interpretation should not be that anxiety is protective. The safer read is that clinic sampling and confounding make simple fear-caries comparisons unstable.
Should dentists screen for dental fear?
Yes. Fear screening can improve communication, appointment planning, analgesia strategy, and adherence even when fear is not the strongest adjusted caries predictor.
What mattered most for caries?
Older age, lower education, and oral hygiene were the most consistent factors in the reported models.
References
- Dental fear, anxiety, oral hygiene and dental caries in Al Ahsa, Saudi Arabia. Nasir and Suliman. doi:10.1007/s44445-026-00153-z
- Dental caries in Saudi Arabia systematic reviews. PubMed search. PubMed search
- Dental anxiety, attendance, and avoidance. PubMed search. PubMed search
- Dental fear, anxiety, and DMFT studies. PubMed search. PubMed search