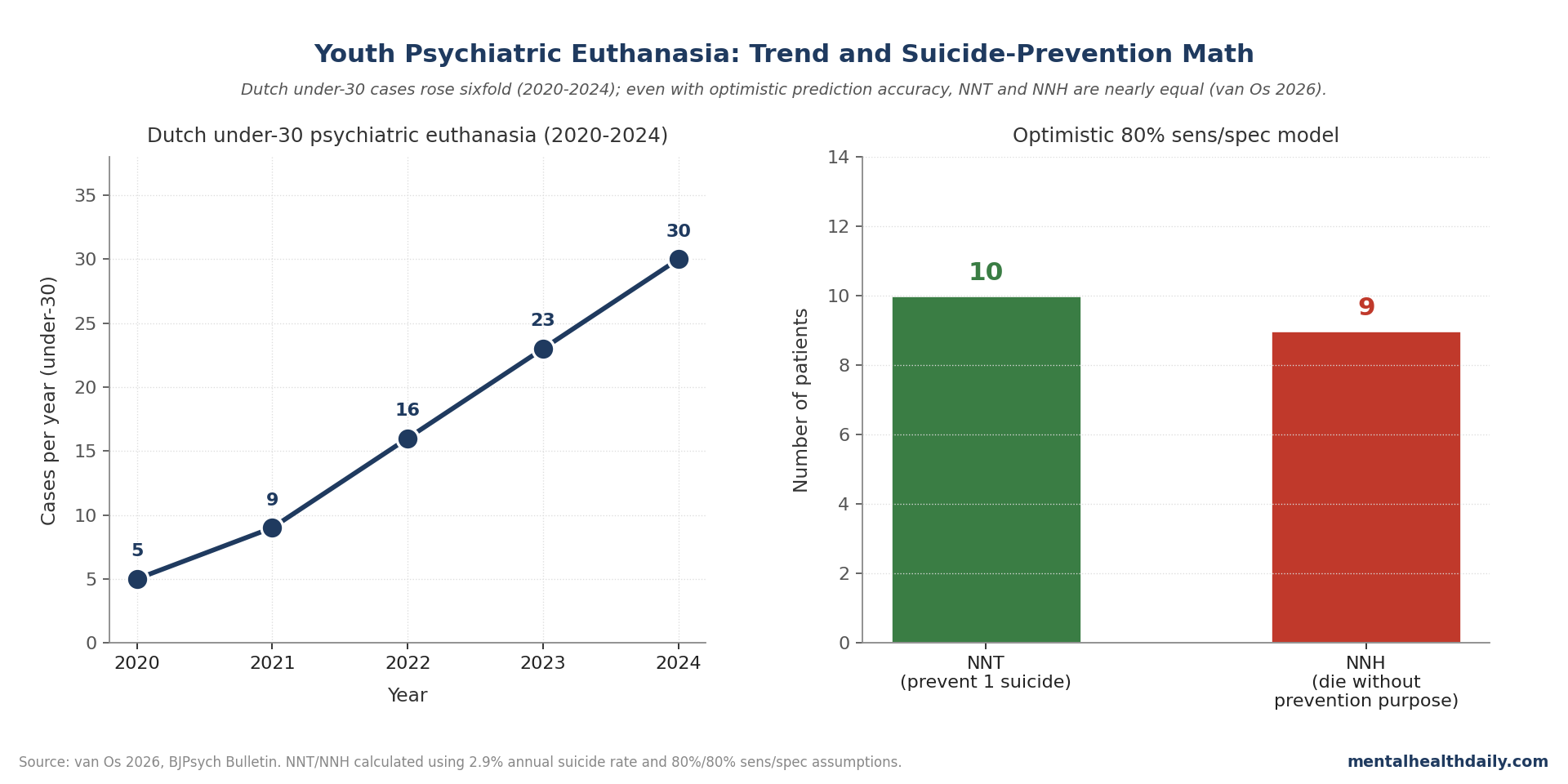
The Netherlands has practiced euthanasia for mental suffering since the early 2000s, and the procedure has expanded rapidly among young people. Between 2020 and 2024, euthanasia procedures for individuals under 30 rose sixfold — from 5 to 30 cases per year — now representing over 9% of all premature deaths (suicide + assisted dying) in that age group. A novel argument has anchored the public debate: that providing assisted dying for psychiatric suffering prevents suicide that would otherwise occur.1
A 2026 BJPsych Bulletin opinion piece by Jim van Os runs the actual numbers on this prevention claim using data from 353 youth applicants at the Dutch Euthanasia Expertise Center. The math is unforgiving. Using optimistic assumptions of 80% sensitivity and 80% specificity for predicting which patients would die by suicide, the analysis returns a number needed to treat (NNT) of 10 to prevent one suicide and a number needed to harm (NNH) of 9. In other words: ten young people would need to undergo assisted dying to prevent one suicide, and nine would die without serving any preventive purpose.1
This is a sensitive topic. The article that follows is a synthesis of the published epidemiological argument, not advocacy. Its goal is to clarify what the suicide-prevention claim does and doesn’t mean when assessed against actual base rates and prediction accuracy.
Research Highlights
- Trend: Dutch under-30 psychiatric euthanasia rose from 5 to 30 cases per year between 2020 and 2024.
- Population studied: 353 youth applicants at Dutch Euthanasia Expertise Center (Schweren et al.).
- Suicide rate in this group: 2.9% annual — roughly fivefold higher than other high-risk psychiatric populations but still far from universal.
- Prediction math: NNT of 10 to prevent one suicide; NNH of 9 (people who die without prevention purpose served).
- Population evidence: Doherty systematic review found no consistent reduction in suicide rates in countries legalizing assisted dying; some saw increases.
- Werther effect concern: Sympathetic media coverage may itself raise suicide risk, undermining any prevention argument.
The Base-Rate Problem Dominates Any Prevention Argument
Suicide is statistically rare even in the highest-risk psychiatric populations. The annual suicide rate among people with treatment-resistant depression is roughly 0.5% — about 5% over a decade. The positive predictive value of suicidal ideation for actual suicide is roughly 4% in psychiatric populations, with an annual suicide risk of 0.3–0.5% among those expressing suicidal thoughts.2
This is not a comfortable finding. It means that most people in the highest-risk psychiatric categories — treatment-resistant depression, expressed suicidal ideation, prior attempts — do not die by suicide. Any clinical or policy framework that equates psychiatric assisted dying with suicide prevention has to confront this base-rate reality before the argument can move forward.
The math is the math: when the underlying event is rare, even very accurate predictors generate large numbers of false positives. This is the foundational problem with screening for any rare event, and it’s the lens through which the suicide-prevention argument has to be evaluated.
The 2.9% Annual Rate in the Specific Applicant Group
The Schweren study tracked 353 youth applicants (under 24) at the Dutch Euthanasia Expertise Center. Among them: 47% withdrew their request, 45% were rejected, 3% died by assisted dying, and 4% died by suicide during the evaluation process — translating to a 2.9% annual suicide risk.3
This is, importantly, a higher base rate than in general psychiatric populations — about fivefold higher than the 0.5% annual rate in treatment-resistant depression. Applicants for euthanasia are not a typical psychiatric sample; they are by definition a self-selected high-risk group.
But 2.9% is still low in absolute terms. For every 100 applicants, roughly 3 will die by suicide in a given year. The remaining 97 will not. Any policy that frames assisted dying as preventing suicide for this group must somehow distinguish, in advance, the 3 from the 97.
Why Optimistic Sensitivity Still Produces Bad NNT
The van Os analysis assumes 80% sensitivity (the procedure correctly identifies 80% of those who would have died by suicide) and 80% specificity (it correctly excludes 80% of those who wouldn’t have). These are extremely optimistic assumptions; real-world prediction accuracy for suicide is far lower.1
Even at 80%/80%, the math returns NNT of 10 and NNH of 9. The Bayesian intuition: when you start with a 2.9% base rate and apply a test with 80% sensitivity and specificity, the positive predictive value remains low because the false-positive rate (20% of the much larger group who weren’t going to die) overwhelms the true-positive rate (80% of the small group who were).
This is the same statistical phenomenon that makes mass screening for rare cancers controversial despite high test accuracy. When the prevalence is low, the number of false positives per true positive grows large, and any irreversible intervention becomes hard to justify on prevention grounds alone.
Population-Level Evidence Doesn’t Support the Prevention Claim
If psychiatric euthanasia genuinely prevented suicide, you’d expect to see suicide rates fall in jurisdictions that legalize the practice. A systematic review by Doherty and colleagues looked at exactly this question across countries that legalized assisted dying for psychiatric or terminal indications. The review found no consistent reduction in suicide rates — and in some jurisdictions suicide rates rose.4
In The Netherlands specifically, despite the rapid growth of psychiatric euthanasia cases, suicide among young women has continued to rise.1 This is the opposite of what a prevention model would predict.
One mechanism proposed for population-level effects in the wrong direction is the Werther effect: media coverage of suicide and suicide-adjacent events can increase subsequent suicide rates, particularly when coverage is sympathetic and provides identification narratives. Romanticized media coverage of psychiatric euthanasia — which the van Os piece notes has occurred in Dutch press — could plausibly contribute to this dynamic.5
What Genuine Suicide Prevention Looks Like
The evidence base for actual suicide prevention is well-established and unrelated to assisted dying. The components include relational continuity in care, trauma-informed treatment, social inclusion, restriction of access to means, treatment of underlying psychiatric illness, and structural factors like economic stability and reduction of isolation.
None of these components are advanced by reframing psychiatric assisted dying as prevention. The prevention framework distracts from interventions with actual evidence and inverts the relationship between care and outcome.
This isn’t an argument about the broader ethics of psychiatric euthanasia, which involve considerations beyond suicide prevention — autonomy, suffering, prognostic certainty, the meaning of “unbearable” suffering, relational and family dynamics, the question of whether psychiatric illness can be considered terminal in the same sense as advanced physical illness. Those debates continue. The narrower point is that the suicide-prevention argument, when run through actual numbers, doesn’t hold.
The Werther Effect and Media Coverage
The Werther effect — named for the wave of imitative suicides following Goethe’s 1774 novel — is well-documented empirically. Sympathetic media portrayal of suicide, particularly with identification-friendly narratives and detailed methodology, increases subsequent suicide rates in measurable ways. WHO and professional society guidelines on responsible reporting exist precisely because of this effect.5
The application to psychiatric euthanasia coverage is contested but the framework is the same: when assisted dying for mental suffering is portrayed as a peaceful, dignified, accessible option for people who feel hopeless, that framing may itself influence vulnerable young people’s thinking. The empirical question of whether this effect contributes to the rising youth suicide rates in the Netherlands is unresolved, but it’s a plausible mechanism that any policy analysis has to consider.
What This Means for Clinical Practice
For clinicians, the takeaway is that the “false negative” argument — the claim that refusing assisted dying to a suicidal patient is dangerous because they might die anyway — doesn’t survive epidemiological scrutiny. The base-rate problem makes prediction unreliable; the population evidence doesn’t support prevention; and the actual suicide-prevention literature points to entirely different interventions.1
This doesn’t resolve the broader ethical questions about psychiatric euthanasia. Reasonable people disagree about autonomy, suffering, and the appropriate scope of medical practice in mental health. The point is narrower: suicide prevention is not the right frame for that ethical debate, and using it as such obscures rather than clarifies what’s at stake.
Common Questions About Psychiatric Euthanasia and Suicide Prevention
Is psychiatric euthanasia legal in the Netherlands?
Yes, since 2002 under specific criteria including unbearable suffering with no prospect of improvement, voluntary and well-considered request, and physician evaluation. Application to psychiatric suffering has expanded over time, and youth applications have grown rapidly in the past five years.
How accurate is suicide prediction in psychiatric care?
Poor. Even sophisticated risk-assessment tools have positive predictive values around 4–6% for suicide in high-risk psychiatric populations. The base-rate problem dominates: most people identified as “high risk” do not die by suicide.
What does the evidence actually support for suicide prevention?
Means restriction (limiting access to lethal methods), continuity of psychiatric care, treatment of underlying conditions, trauma-informed care, and social/relational support. Population-level interventions like firearm restrictions in the US and barriers on suicide hotspots have measurable effects.
Is this debate happening outside the Netherlands?
Yes. Belgium, Canada, and Switzerland all permit some form of assisted dying that includes or may include psychiatric indications. Each jurisdiction has its own evolving legal framework and ethical debate.
This article discusses suicide and assisted dying as policy and epidemiology topics. If you or someone you know is struggling with thoughts of suicide, support is available through national crisis lines and mental health services.
References
- van Os J. The Dutch debate on youth psychiatric euthanasia and suicide prevention. BJPsych Bulletin. 2026;doi:10.1192/bjb.2026.10231.
- Large M et al. Meta-analysis of longitudinal cohort studies of suicide risk assessment. PLOS One. 2016;11(6):e0156322. doi:10.1371/journal.pone.0156322
- Schweren LJS, Rasing SPA, Kammeraat M, et al. Requests for medical assistance in dying by young Dutch people with psychiatric disorders. JAMA Psychiatry. 2025;82(3):246–252. doi:10.1001/jamapsychiatry.2024.4006
- Doherty AM et al. Assisted dying and suicide rates: a systematic review. BJPsych Bull. 2023. doi:10.1192/bjo.2022.71
- Sisask M, Värnik A. Media roles in suicide prevention: a systematic review. Int J Environ Res Public Health. 2012;9(1):123-138. doi:10.3390/ijerph9010123