
Brief screening tools for early dementia risk are essential in primary care. A 2026 study by You et al. evaluated the AD8 informant questionnaire in older Chinese-speaking adults in Australia, mapping how cognitive, functional, social, and language-barrier risks stack before dementia is formally diagnosed.1
Research Highlights
- The AD8 dementia screening interview is an 8-item informant-based questionnaire that takes about 3 minutes to complete and discriminates non-demented from mildly demented older adults.2
- The 2026 AD8 study tested older Mandarin/Cantonese-speaking adults in Australia — a population at elevated dementia risk that can be missed by English-only screening pathways.1
- Pre-dementia indicators measured by AD8 cluster with multiple vulnerability domains: cognitive, functional, social, and language-barrier-related factors.1
- Cultural and linguistic adaptation of dementia screening matters: tools validated in English-speaking populations may have different operating characteristics in non-English-speaking immigrant communities.3
- Implication for primary care: early identification of cognitive decline in linguistic-minority older adults supports earlier intervention and access to culturally-appropriate dementia services.1
Dementia diagnosis is often delayed in immigrant older adults, with multiple contributing factors: language barriers to clinical assessment, cultural differences in symptom expression, and limited specialist access.3,4
The Mayeda et al. analysis of Kaiser Permanente Northern California data is one of the more striking demonstrations of the problem. Across 14 years of follow-up, the incidence of dementia in Black older adults was 65% higher than in non-Hispanic white older adults; American Indian/Alaska Native older adults showed similar elevated incidence.
Asian American and Hispanic/Latino older adults showed intermediate patterns that varied by subgroup. These differences persisted after adjusting for cardiovascular and metabolic risk factors, suggesting that the gap reflects both differential exposure to known dementia risk factors and unequal access to diagnostic and preventive care that would catch cases earlier.6
The AD8 was designed for rapid informant-based screening and has been translated into multiple languages with demonstrated psychometric validity. This study extended that work by examining how AD8 performance integrates with broader vulnerability domains in older Chinese-speaking immigrants.
The original Galvin et al. validation showed that AD8 has roughly 84% sensitivity and 80% specificity for detecting dementia at the 2-or-higher cutoff, with administration times consistently under 5 minutes. This puts AD8 in the “brief screening” tier alongside Mini-Cog, which adds clock-drawing and 3-item recall to a few orientation questions.
The informant-based design is particularly useful when patients themselves are unable to engage extensively with cognitive testing — due to language, cultural, or sensory barriers, or because the patient’s impairment includes anosognosia (lack of awareness of their cognitive change). Family caregivers often have observational access to subtle functional changes that brief patient-facing tests miss.2
AD8 Screening in Mandarin- and Cantonese-Speaking Adults
You et al. recruited older Mandarin- and Cantonese-speaking adults through Australian community organizations, including Chinese Australian Services Society and Arabic Council Australia. AD8 was administered alongside additional measures of cognitive, functional, social, and demographic vulnerability.1
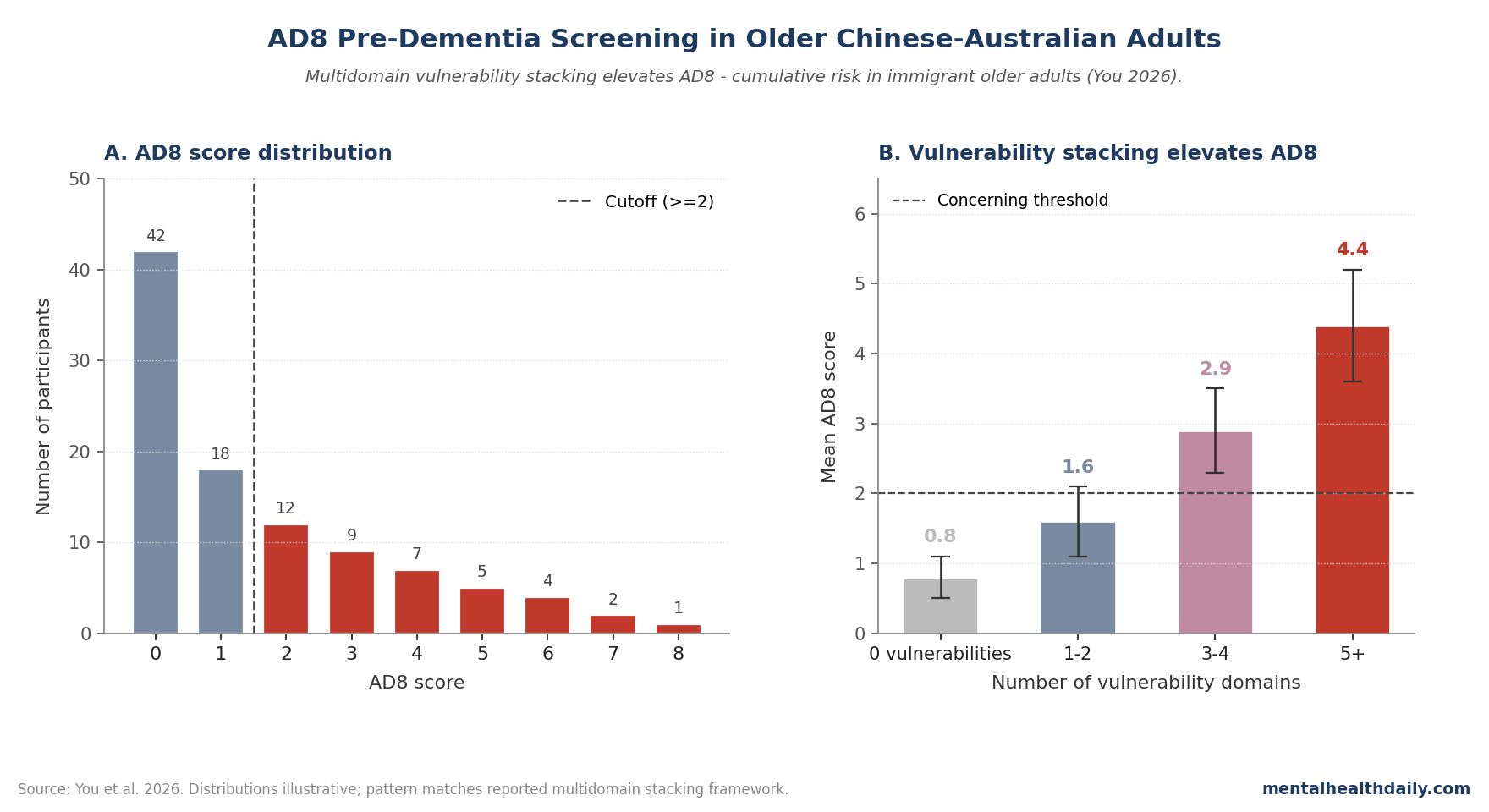
The results had 2 clinically useful patterns:
- AD8 produced interpretable screening variation. Scores varied enough to separate lower-risk from higher-risk participants instead of collapsing into a useless narrow range.
- Cumulative vulnerability stacked risk. Lower socioeconomic status, limited English proficiency, functional decline, and social isolation each tracked higher AD8 scores; multiple vulnerabilities together produced substantially higher scores than single risk factors.1
The cultural-competence dimension of the implementation deserves attention. The study used Mandarin- and Cantonese-language administration with cultural-liaison support during recruitment, partnering with the Chinese Australian Services Society for community trust-building.
AD8’s informant-based design fits Chinese family caregiving norms reasonably well, where adult children are often deeply involved in older-parent health and well-positioned to notice cognitive change. The same design might function differently in cultures where elder-care is more institutionalized or where extended-family dynamics differ.
Linguistic adaptation alone is necessary but not sufficient; community partnership and culturally-aligned administration matter for screening reach.1,3
Multidomain Screening Catches Risk AD8 Alone Can Miss
Single-test screening misses much of the contextual variation that contributes to dementia risk in immigrant older adults. AD8 captures observable functional and cognitive change but doesn’t directly measure language, social, or financial vulnerabilities. Combining AD8 with broader risk questions creates a fuller picture of who needs dementia-relevant follow-up.1,5
The vulnerability-stacking pattern fits a broader literature on cumulative-risk models in geriatrics. Frailty research has long emphasized that single deficits are weakly predictive whereas counts of accumulated deficits across multiple domains produce robust outcome prediction.
The Pre-Dementia AD8 framework operates by similar logic: any one of socioeconomic disadvantage, language barrier, functional decline, or social isolation is modestly informative; the combination is strongly informative.
This has practical implications for primary-care screening protocols, which can incorporate brief social-determinant questions alongside cognitive screening at minimal additional time cost while substantially improving the yield of the overall assessment.5
The screening picture has 3 separable layers:
- Cognitive/functional — what AD8 directly measures.
- Linguistic/cultural — capacity to access English-language clinical services and educational materials.
- Social/economic — isolation, financial stress, family caregiving capacity.
What This Adds to Dementia Risk Screening
Dementia risk screening has a practical access problem: older adults who do not move easily through English-language clinics may be diagnosed later, receive less specialist care, and miss the window where family planning and risk-factor management are most useful.4,6
The useful contribution here is operational: brief informant-based screening can be deployed in non-English-speaking immigrant communities through community-organization partnerships, with culturally-aligned administration and a clearer path from risk flag to clinical follow-up.1
Limitations of This AD8 Screening Analysis
Three caveats deserve weight:
- Cross-sectional design. Whether AD8 in this population predicts future dementia conversion is the next required validation.
- Single ethnic-linguistic group. Generalizability to other immigrant populations needs separate testing — cultural and linguistic factors vary substantially across communities.
- Recruitment through community organizations may oversample socially-engaged older adults and undersample the most isolated — a group that may have the greatest screening-access problem.
Screening Is Not Diagnosis, and Translation Is Not Enough
Two distinctions matter:
- AD8 is a screening tool, not a diagnostic test. Elevated AD8 scores indicate concern but require formal assessment for diagnosis. Coverage that conflates the two oversells the framework’s clinical reach.2
- Dementia screening in non-English-speaking populations is not only a translation problem. Cultural variation in symptom expression, family-based caregiving, and willingness to discuss cognitive concerns all affect screening sensitivity. Linguistic adaptation is necessary but not sufficient.3
Mandarin/Cantonese AD8 Screening Needs Referral Pathways
For clinicians serving non-English-speaking older adults, the results support the use of AD8 in Mandarin and Cantonese as a brief screening tool, with cultural-liaison support during administration. For health systems, the multidomain vulnerability framework supports broader risk screening alongside cognitive screening for high-risk populations.1,5
Implementation deserves attention beyond the screening tool itself. Successful deployment requires bilingual or interpreter-supported clinical encounters, clear pathways from positive screen to specialist evaluation that don’t require English fluency at every step, and culturally competent dementia education for families considering further evaluation.
The Pre-Dementia work suggests that screening alone — even validated, multidomain, culturally adapted screening — is insufficient if the downstream system isn’t prepared to receive positive screens. Community-organization partnerships of the kind used in this study provide one model: trusted community institutions handle initial screening and family education, with structured referral to mainstream clinical services for evaluation.1,3
Questions About Dementia Screening
What is the AD8?
An 8-item informant-based interview that asks a family member or close contact whether the older adult shows specific changes in memory, judgment, and daily function. It takes about 3 minutes and produces a 0-8 score. The 8 items cover problems with judgment, reduced interest in hobbies/activities, repeating questions, trouble learning new tools, forgetting the month or year, trouble handling complicated financial affairs, trouble remembering appointments, and consistent problems with thinking or memory.2
What score is concerning?
An AD8 score of 2 or higher is the standard cutoff for further dementia evaluation in most validation studies, though optimal thresholds vary by population. The score itself isn’t a diagnosis — it’s a flag that prompts more thorough cognitive evaluation including formal neuropsychological testing, brain imaging where indicated, and laboratory workup for reversible causes.2
Why is dementia screening difficult in immigrant populations?
Language barriers, cultural differences in expressing cognitive concerns, family-based caregiving norms, and reduced access to specialist services all contribute. Screening tools validated in majority populations may miss cases or produce false positives.3
How does this fit with global dementia prevention?
The Lancet Commission on dementia prevention identifies modifiable risk factors and supports population-level interventions. Language-aware risk screening complements this by identifying at-risk people who might otherwise be missed. Without case-finding that reaches non-English-speaking older adults, prevention frameworks stay easier to use for people already well served by the health system.5
Is AD8 better than other screening tools?
AD8 has strengths (brief, informant-based, doesn’t depend on patient cognitive performance during testing) and limitations (depends on availability of an informant, doesn’t directly assess the patient). Tools like Mini-Mental State Examination and Montreal Cognitive Assessment add complementary information. Combining informant-based and patient-administered tools produces better screening sensitivity than either alone, particularly in patients whose cognitive change is subtle or whose insight into their own cognition is reduced by anosognosia.2
Should families seek out AD8 testing?
If concerns about cognitive change in an older relative arise, primary-care discussion with appropriate screening (AD8 or alternatives) is reasonable. AD8 itself is freely available and brief; it’s typically administered in clinic. Family members can also use AD8 informally as a structured way to organize their own observations before bringing them to a clinical appointment, helping ensure that subtle changes don’t get lost in a brief visit.2
What’s the next study that needs to happen?
Longitudinal validation of AD8 in this population (predicting actual dementia conversion), expansion to other immigrant communities, and integration with language, social, and functional risk assessment for comprehensive risk stratification.
References
- You W, Koo FK, Cheng Y, et al. Pre-dementia indicators and multidomain vulnerabilities: insights from AD8 screening in older Chinese-speaking adults. Geriatrics & Gerontology International / Journal of Cross-Cultural Gerontology. 2026. doi:10.64898/2026.04.08.26350424
- Galvin JE, Roe CM, Powlishta KK, et al. The AD8: a brief informant interview to detect dementia. Neurology. 2005;65(4):559–564. doi:10.1212/01.wnl.0000172958.95282.2a
- Cooper C, Tandy AR, Balamurali TBS, Livingston G. A systematic review and meta-analysis of ethnic differences in use of dementia treatment, care, and research. American Journal of Geriatric Psychiatry. 2010;18(3):193–203. doi:10.1097/jgp.0b013e3181bf9caf
- Mukadam N, Cooper C, Livingston G. A systematic review of ethnicity and pathways to care in dementia. International Journal of Geriatric Psychiatry. 2011;26(1):12–20. doi:10.1002/gps.2484
- Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396(10248):413–446. doi:10.1016/s0140-6736(20)30367-6
- Mayeda ER, Glymour MM, Quesenberry CP, Whitmer RA. Inequalities in dementia incidence between six racial and ethnic groups over 14 years. Alzheimer’s & Dementia. 2016;12(3):216–224. doi:10.1016/j.jalz.2015.12.007