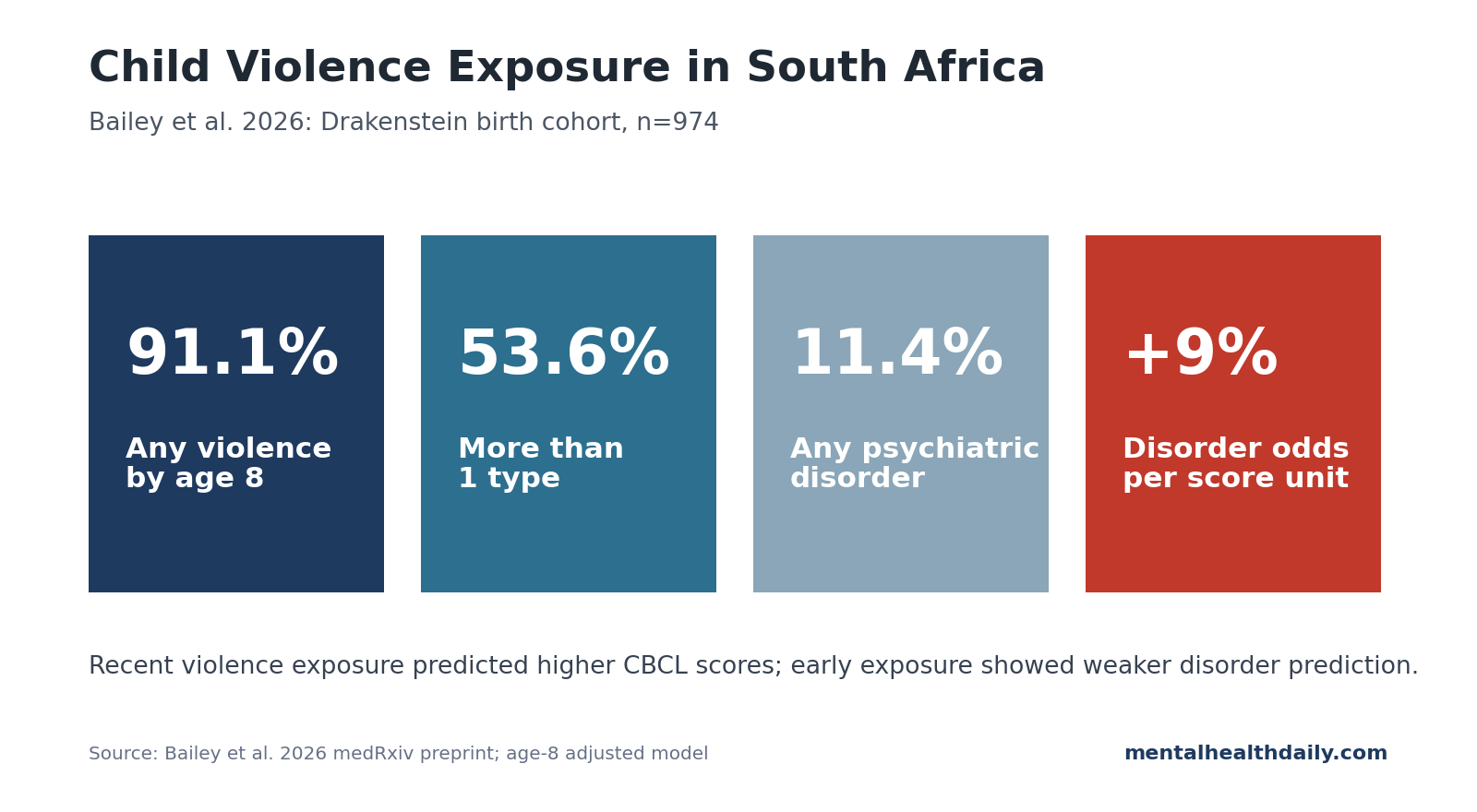
Violence exposure was nearly universal by age 8 in a South African birth cohort: 91.1% of children had experienced at least 1 violence type, and 53.6% had experienced more than 1. Recent violence exposure at age 8 was consistently tied to mental-health problems, while earlier exposure at age 4.5 showed weaker longitudinal prediction than same-age exposure at age 8.1
Research Highlights
- Violence exposure was extremely common: 75.4% of children had exposure by age 4.5, rising to 91.1% by age 8 in the Drakenstein Child Health Study.1
- Recent exposure tracked symptoms: At age 8, each 1-unit increase in total violence score predicted higher CBCL total, internalizing, and externalizing scores after adjustment.1
- Psychiatric disorder odds increased: Each 1-unit increase in total age-8 violence score was associated with 9% higher odds of any psychiatric disorder (aOR 1.09, 95% CI 1.05-1.13).1
- Early exposure was less predictive: Violence exposure by age 4.5 predicted later CBCL scores modestly, but did not predict any psychiatric disorder at age 8 (aOR 1.00, 95% CI 0.93-1.06).1
- Domestic violence looked especially consequential: Domestic victimization predicted symptoms longitudinally, and witnessing domestic violence showed one of the strongest cross-sectional links to disorder.1
The result keeps the focus on timing, recurrence, and proximity to the mental-health assessment, especially in high-violence settings where exposure is common rather than exceptional.
Bailey et al. Analyzed 974 South African Children Followed to Age 8
Bailey et al. analyzed 974 children from the Drakenstein Child Health Study, a South African birth cohort from a peri-urban area near Cape Town. Violence exposure was assessed at ages 4.5 and 8 using caregiver and child reports, while mental health at age 8 was measured with caregiver-reported Child Behavior Checklist (CBCL) scores and the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID).1
CBCL means stayed below 50, and 11.4% of children met criteria for at least 1 psychiatric disorder at age 8. That combination is important: violence exposure was widespread, while the main signal was a graded increase in risk within a high-exposure population.
The design improves on much of the violence literature because it used a birth cohort, multiple violence types, child and caregiver reports, and structured diagnostic interviewing. But the 2026 paper is still a medRxiv preprint, so details may change after peer review.
The cohort framing also helps separate prevalence from prediction. The study asked whether earlier exposure predicted later symptoms, whether recent exposure was more tightly linked to current symptoms, and whether specific violence types carried different risk signals.
Recent Violence Exposure Predicted More Mental-Health Problems
Cross-sectional age-8 results were the strongest part of the paper. In fully adjusted models that also controlled for earlier CBCL total score, each 1-unit increase in total violence exposure at age 8 predicted higher age-8 CBCL scores:
- Total problems: B = 0.49 (95% CI 0.32-0.66), p < 0.001.
- Internalizing problems: B = 0.32 (95% CI 0.17-0.47), p < 0.001.
- Externalizing problems: B = 0.46 (95% CI 0.31-0.61), p < 0.001.
The diagnostic model pointed in the same direction. Each 1-unit increase in total violence score was associated with 9% higher odds of any psychiatric disorder at age 8 (aOR 1.09, 95% CI 1.05-1.13).1
The per-unit effect is modest, but the exposure scale accumulates. In a setting where more than half of children had experienced multiple violence types by age 8, small increments can become meaningful at the population level.
Early Exposure Was Weaker Than Same-Age Exposure
The longitudinal findings were more modest. Violence exposure at age 4.5 predicted age-8 CBCL total, internalizing, and externalizing scores, but the coefficients were smaller: B = 0.27, 0.24, and 0.23, respectively, after adjustment for confounders and earlier CBCL total score.1
For psychiatric disorder diagnosis, earlier total violence exposure did not predict age-8 disorder status: aOR 1.00 (95% CI 0.93-1.06), p = 0.922. None of the violence subscales or polyvictimization predicted disorder in that fully adjusted longitudinal model.
The most grounded interpretation is proximity. Recent violence may be more tightly coupled to current symptoms because it is still shaping stress physiology, family routines, school behavior, sleep, and perceived safety. Earlier exposure can still matter, especially when repeated or domestic, but its signal is harder to isolate after later exposures accumulate.
Screening should separate lifetime vulnerability from current safety. A lifetime violence checkbox can identify broad vulnerability, but it does not tell a clinician whether the child is currently unsafe, recently destabilized, or living in a household where violence remains active. The Bailey data point toward that more granular question.
Domestic Victimization Was the Most Consistent Longitudinal Signal
Violence type mattered. Witnessed community violence was the most common exposure at both ages, reaching 74.7% by age 8. But community violence was not the strongest predictor of diagnosed disorder after adjustment, and its age-8 association with any disorder weakened to aOR 1.07 (95% CI 0.99-1.15), p = 0.080.1
Domestic victimization was more consistent. At age 4.5, domestic victimization predicted all 3 age-8 CBCL domains even after adjustment. At age 8, domestic victimization was associated with higher total, internalizing, and externalizing scores and higher odds of disorder.
Witnessing domestic violence also showed a strong same-age disorder association: aOR 1.52 (95% CI 1.23-1.87) after controlling for confounders and earlier CBCL score. In plain terms, violence inside the child’s close relational world looked more clinically concentrated than community exposure alone.
Community violence still deserves attention.
Domestic exposure: threat from people or spaces that should be protective may carry a different psychological load, with reduced recovery time and less separation between danger and ordinary family life. Those mechanisms are plausible, but the study itself tested associations, not mechanisms.
Broader childhood adversity literature: The Bailey findings fit a large literature linking childhood maltreatment, community violence, domestic violence, and polyvictimization with later mental-health problems. Meta-analytic work has found robust associations between childhood maltreatment and psychiatric outcomes, while community-violence meta-analysis links exposure to emotional distress and behavioral problems in children and adolescents.2,5
What this South African cohort adds is setting and timing. Much of the longitudinal evidence comes from high-income countries and single-exposure frameworks. The Drakenstein data show that in a low- and middle-income country context with very high exposure prevalence, the key question is not “was there any violence?” It is which type, how recent, how repeated, and whether it occurred inside the household.
This also guards against a common overread. High exposure prevalence and deterministic framing are different things. In this cohort, 11.4% met criteria for any psychiatric disorder at age 8. Violence exposure raised risk; it did not make disorder inevitable.
Limits of the South African Birth-Cohort Evidence
- The preprint is not peer-reviewed. The results are detailed and useful, but the final journal version may revise methods, tables, or interpretation.
- Cross-sectional associations can run both ways. Current mental-health problems may increase risk of violence exposure, caregiver reporting, or both.
- Violence reports can be incomplete. Caregivers may miss community experiences, and children may underreport domestic violence because of fear, shame, or normalization.
- Exposure scores combine frequency and type. A 1-unit increase has statistical meaning inside the model, but it is not a simple clinical unit like 1 event.
Child Mental-Health Prevention Should Prioritize Recent and Domestic Exposure
For children living in high-violence settings, mental-health screening should ask about recent exposure, repeated exposure, domestic victimization, and lifetime trauma history.
For prevention, domestic violence and caregiver-child safety deserve special weight because they are both clinically concentrated and potentially modifiable through family, school, legal, and community interventions. Community violence still matters, but domestic exposure appears to carry a sharper signal for child psychopathology in this cohort.
A generic adverse-childhood-experiences score is too blunt for this setting. In high-exposure communities, the actionable questions are which exposures are still happening, which adult can protect the child, and whether the child’s current symptoms fit an active safety problem rather than a remote history.
Questions About Child Violence Exposure and Mental Health
Does this prove violence caused the psychiatric disorders?
No. The strongest findings were same-age associations, and cross-sectional models cannot prove direction. The longitudinal results support a weaker prospective signal than the age-8 same-age models, especially for domestic victimization.
The safest read is risk amplification, not clean causality. Violence exposure and child symptoms can reinforce each other through family stress, school problems, sleep disruption, and caregiver reporting.
Why were disorder rates not higher if 91.1% had violence exposure?
Exposure raises risk but does not determine outcome. Protective relationships, school structure, temperament, community support, and measurement limits all shape whether a child develops a diagnosable disorder.
Which violence type looked most important?
Domestic victimization was the most consistent longitudinal signal, while witnessing domestic violence showed one of the strongest same-age disorder associations. Witnessed community violence was more common but less specific.
What should clinicians ask?
Ask about recent violence, violence at home, repeated exposure, school victimization, sleep, behavior change, and whether the child has a safe adult. Lifetime trauma checklists miss the timing and proximity that mattered here.
For a child who screens positive, the next step is checking current safety, caregiver support, school functioning, and whether symptoms are internalizing, externalizing, or both.
References
- Bailey M, Hammerton G, Fairchild G, et al. Violence exposure and mental health problems among school-aged children in a South African birth cohort. medRxiv preprint. 2026. doi:10.64898/2026.04.20.26351289
- Baldwin JR, Wang B, Karwatowska L, et al. Childhood maltreatment and mental health problems: a systematic review and meta-analysis of quasi-experimental studies. American Journal of Psychiatry. 2023;180(2):117-126. doi:10.1176/appi.ajp.20220174
- Carr A, Duff H, Craddock F. A systematic review of reviews of the outcome of noninstitutional child maltreatment. Trauma, Violence, & Abuse. 2020;21(4):828-843. doi:10.1177/1524838018801334
- Ribeiro WS, Andreoli SB, Ferri CP, Prince M, Mari JJ. Exposure to violence and mental health problems in low and middle-income countries: a literature review. Brazilian Journal of Psychiatry. 2009;31(Suppl 2):S49-S57. doi:10.1590/s1516-44462009000600003
- Fowler PJ, Tompsett CJ, Braciszewski JM, Jacques-Tiura AJ, Baltes BB. Community violence: a meta-analysis on the effect of exposure and mental health outcomes of children and adolescents. Development and Psychopathology. 2009;21(1):227-259. doi:10.1017/s0954579409000145
- Tsunga L, Lake M, Halligan SL, et al. Early childhood violence exposure patterns in the Drakenstein Child Health Study. Wellcome Open Research. 2023;8:36. doi:10.12688/wellcomeopenres.18598.2
- Tsunga L, Heron J, Lake MT, et al. Exposure to violence and mental health outcomes among pre-schoolers in a South African birth cohort. Research on Child and Adolescent Psychopathology. 2024;52:1635-1646. doi:10.1007/s10802-024-01211-y